.avif)
.svg)
.svg)
How payer algorithms are reducing your billing codes without reading the chart, what the major commercial and Medicare Advantage programs do, and how to detect, appeal, and prevent it.
Payer downcoding is the practice of an insurer reducing a physician-submitted billing code to a lower-level, lower-paying code - cutting reimbursement even when the higher level of care was delivered and documented. It is an old problem that has become a new one, because it is now overwhelmingly automated: payer algorithms and AI reduce the code without an individual review of the medical record, reading structured claim data, comparing it against peer-coding benchmarks or a proprietary payment matrix, and reassigning the code in seconds. The practice most often targets high-level evaluation and management (E/M) codes - reducing a documented 99214 or 99215 to a 99213 - and it has moved from an occasional irritant to a routine cost-containment strategy across nearly every major insurer. The financial drain is significant: industry estimates put the cost at $40,000 to $180,000 per practice per year.
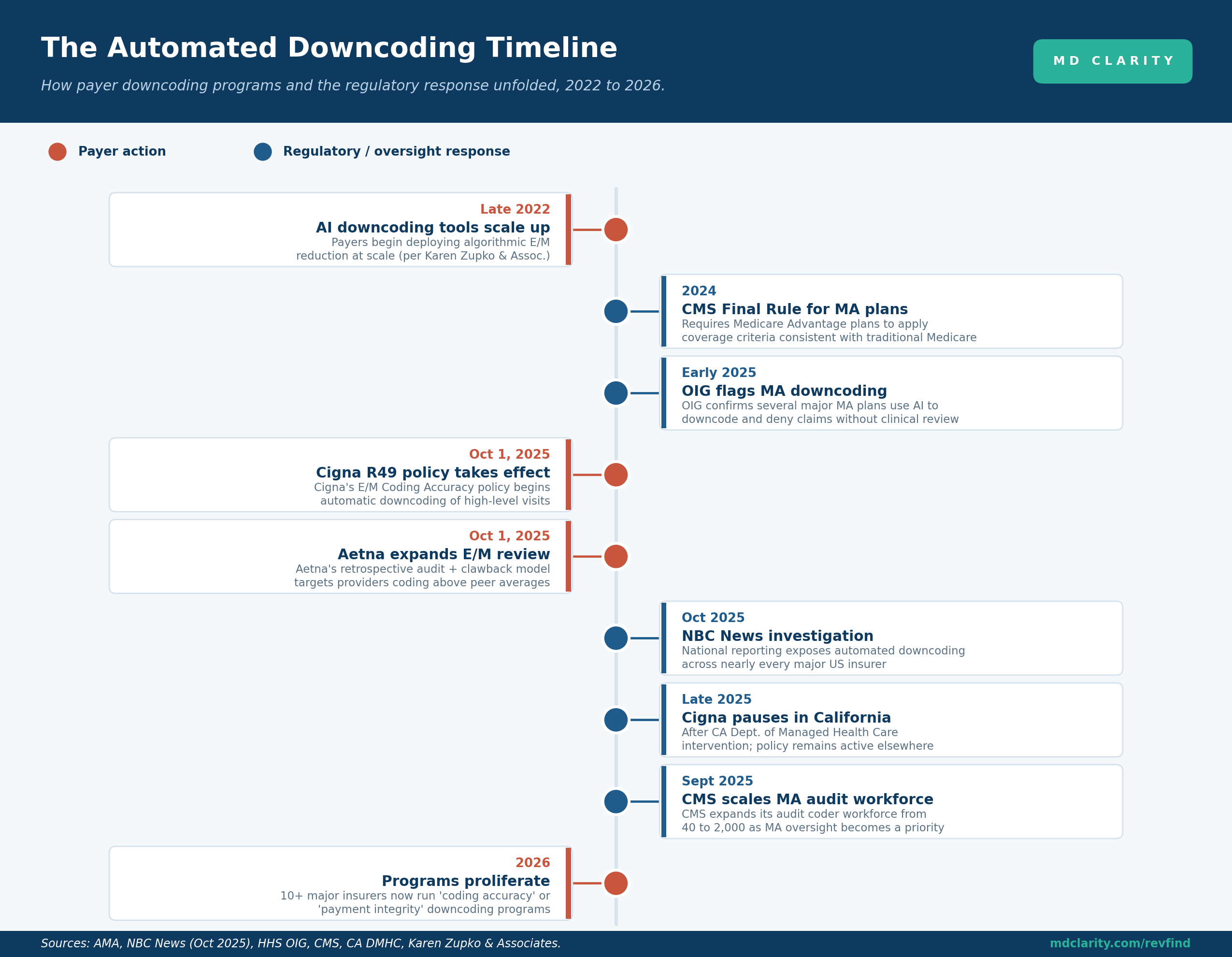
The practice scaled quietly. According to a 2025 white paper by Karen Zupko & Associates, payers including UnitedHealthcare, Cigna, Aetna, and regional Blue Cross Blue Shield plans began deploying AI-driven downcoding tools at scale starting in late 2022. By October 2025, an NBC News investigation found automated downcoding had expanded across nearly every major US insurer. The same month, Cigna's E/M Coding Accuracy policy (commonly referenced by its R49 designation) took effect, and Aetna expanded its E/M review program. The regulatory response is now catching up, but the operational burden has already landed squarely on provider revenue cycles.
Key takeaways
- Automated downcoding reduces your code without reading the chart. Algorithms reassign high-level E/M codes based on structured data and peer benchmarks, not clinical documentation.
- It is now nearly universal. More than ten major insurers run "coding accuracy" or "payment integrity" downcoding programs as of 2026, including Cigna, Aetna, UnitedHealthcare, Humana, Elevance, and regional Blues plans.
- Medicare Advantage is a major front. HHS OIG confirmed in 2025 that several MA plans use AI to downcode without adequate clinical review. Accepting a downcode without appeal can even create False Claims Act exposure.
- It hides as an adjustment, not a denial. Because downcodes post as payment adjustments, they never appear on denial reports. Only a submitted-code-versus-paid-code variance check reliably surfaces them.
- Your documentation is your defense. Records that satisfy the 2021 AMA E/M criteria for the billed code are the foundation of every appeal, across both commercial and MA programs.
- The cost is real. $40,000 to $180,000 per practice annually, at $45 to $80 per downcoded office visit and $3,000 to $7,000 per inpatient DRG downgrade.
What is on this page
- What is payer downcoding?
- Why automated downcoding is exploding now
- How automated downcoding actually works
- The major commercial payer programs
- Medicare Advantage downcoding: a distinct and growing front
- The financial impact by specialty
- How to detect automated downcoding
- How to appeal and recover
- How to prevent it going forward
- How MD Clarity helps
- FAQ
What is payer downcoding?
Downcoding happens when a payer reimburses a claim at a lower level of service than the one the provider billed. You submit a claim for a high-complexity visit (say, CPT 99215), and the payer processes and pays it as a 99213. The difference between what you documented and what you were paid is lost revenue.
Automated downcoding is the version of this practice carried out by software rather than a human reviewer. Instead of a clinician or certified coder examining the medical record and forming a judgment, an algorithm scans the structured fields on the claim - diagnosis codes, time fields, the relationship between the presenting problem and the billed level - and makes a reduction decision in seconds. Most of these systems never look at the actual clinical documentation.
It is worth distinguishing a few related terms:
- Downcoding is payer-initiated. The payer reduces the code you submitted.
- Undercoding is provider-initiated. A coder conservatively assigns a lower code than the documentation supports, often to avoid a denial.
- Upcoding is the opposite of downcoding and a compliance violation: billing for a more complex service than was documented.
- Underpayment is the broader category. A claim can be underpaid even when the code is accepted as submitted, simply because the payment does not match the contracted rate. Downcoding is one specific mechanism that produces underpayment.
The through-line for revenue cycle teams: automated downcoding is a form of underpayment that is uniquely hard to see, because the code change is buried in an adjustment rather than flagged as a denial.
Why automated downcoding is exploding now
Several forces converged to make automated downcoding a default payer strategy rather than an occasional one.
The 2021 E/M guideline changes. When the AMA revised the office-visit E/M guidelines in 2021 to allow code selection based on medical decision-making (MDM) or total time, legitimate Level 4 and Level 5 coding increased. Payers interpreted the rise as an opportunity for scrutiny rather than evidence of accurate documentation, and built algorithms to push those levels back down.
Cost containment through AI adjudication. AI-powered claim adjudication lets payers cut claim costs in real time at enormous scale. A payer algorithm can scan and adjust thousands of claims per second, far faster than any provider compliance team can review them.
Peer comparison benchmarking. Many programs work by flagging providers whose coding distribution trends above peer averages, then reducing the outliers, regardless of whether the higher coding was clinically justified. A practice that genuinely sees more complex patients looks like an outlier and gets penalized for it.
The subjectivity of E/M. E/M services rely on documentation of MDM or time, both of which involve interpretation. That subjectivity makes E/M claims uniquely vulnerable to algorithmic second-guessing in a way that, say, a fixed-price procedure is not.
How automated downcoding actually works
Understanding the mechanism is what makes detection and appeal possible. The process is fast, automated, and - critically - skips the one step that would make it defensible.
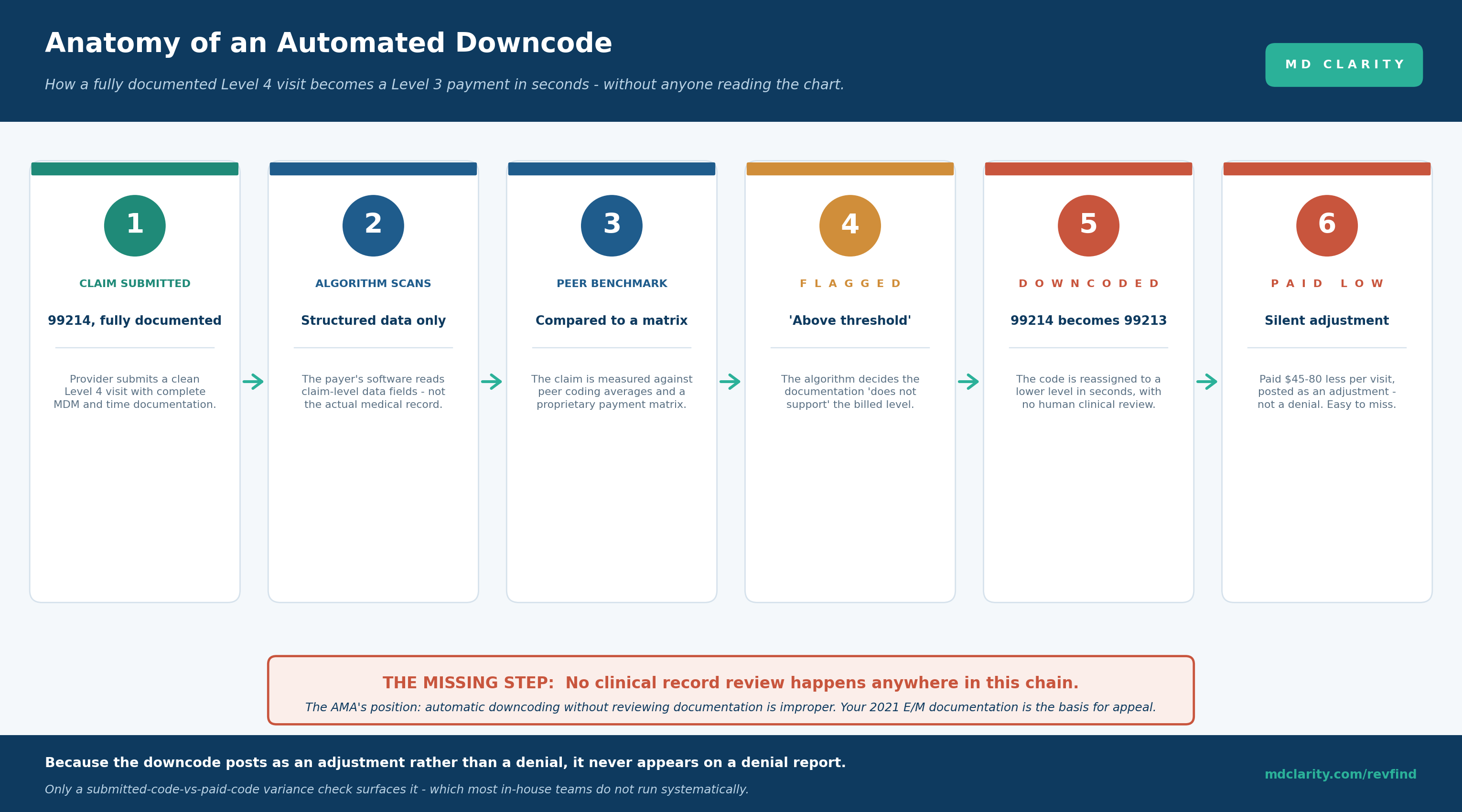
The provider submits a clean, fully documented Level 4 claim. The payer's algorithm reads the structured claim data - not the medical record. It compares the claim against peer-coding averages and a proprietary payment matrix. It decides the documentation "does not support" the billed level and flags the claim as above threshold. The code is reassigned to a lower level. The claim is paid at the lower rate, posted as an adjustment rather than a denial.
The missing step is the one that matters: no clinical record review happens anywhere in this chain. The AMA's position is explicit - automatic or algorithm-driven downcoding without adequate clinical review and provider notification is improper. National medical organizations have asked payers to target downcoding only at true outlier providers, conduct medical record review before adjustment, provide advance notice, and communicate clearly about appeal options. Most automated programs do none of these.
Because the downcode posts as an adjustment, it never appears on a denial report. A practice watching its denial rate can see that number hold steady or even improve while automated downcoding quietly drains revenue underneath it. Only a submitted-code-versus-paid-code variance check surfaces the problem - and most in-house teams do not run that check systematically.
The major commercial payer programs
The largest commercial insurers have each taken a somewhat different approach to automated downcoding. Knowing the specifics shapes how you respond to each.
Cigna's E/M Coding Accuracy policy (R49)
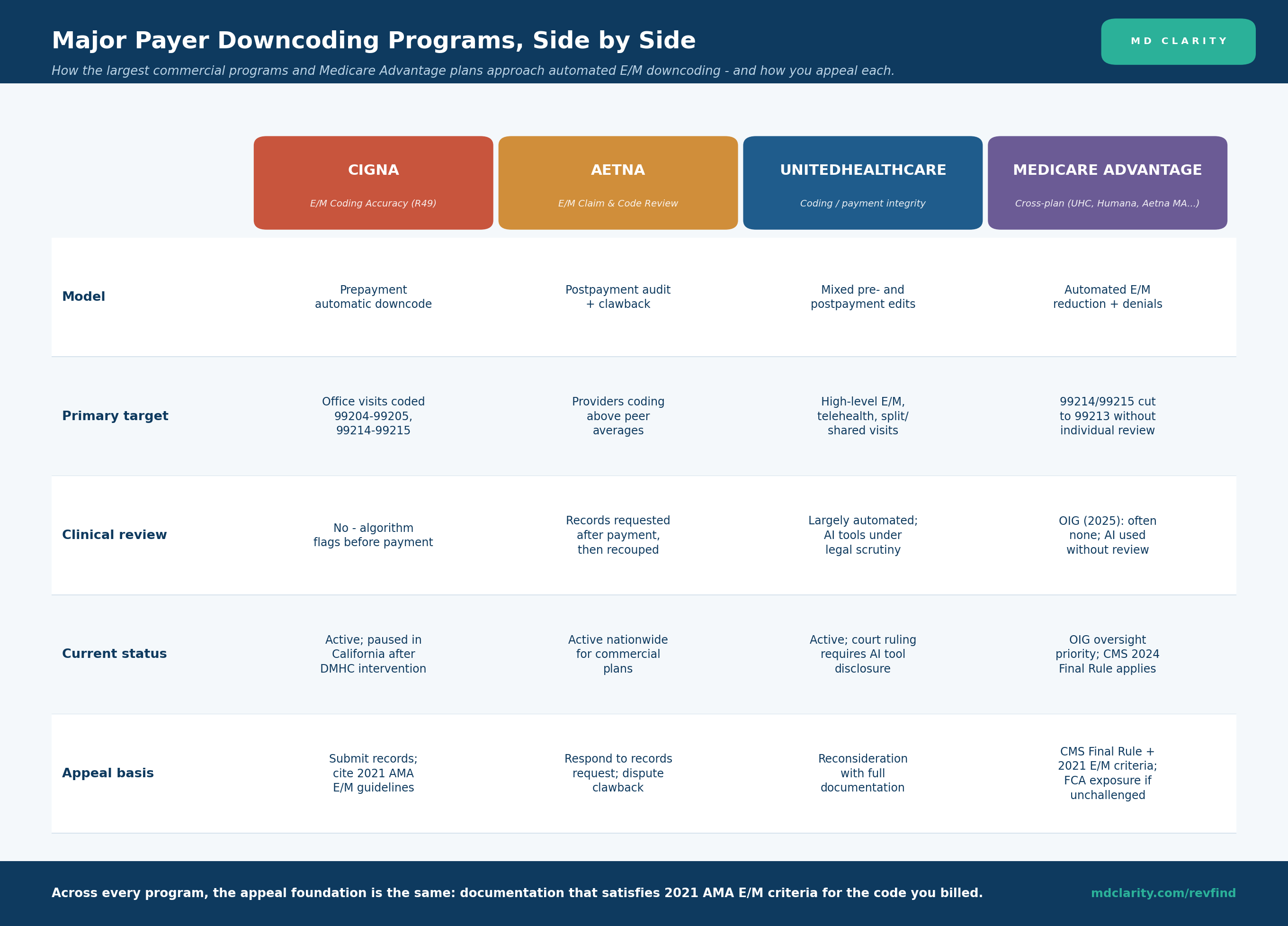
Cigna's policy, effective October 1, 2025, enables automatic downcoding of higher-level E/M services when its proprietary algorithm determines the documentation does not support the billed level - frequently without examining the actual medical record. It operates on a prepayment basis: the code is reduced before payment goes out.
The policy drew significant pushback. Following intervention by the California Department of Managed Health Care, Cigna agreed to pause implementation in California. The policy remains active in other states, which means a multistate group may see Cigna downcodes in some markets but not others - a pattern worth tracking by location.
Aetna's E/M Claim and Code Review Program
Aetna relies more heavily on a postpayment model. Under its E/M Claim and Code Review Program, commercial plans nationwide conduct retrospective reviews targeting "overutilizers" - providers whose coding patterns trend above peer averages. Providers initially receive full reimbursement, then face clawbacks weeks or months later when Aetna requests documentation. Even when the notes justify the higher codes, practices face delays and administrative burden to restore the payment.
The postpayment model is operationally different from prepayment downcoding: the money arrives and then leaves, which can distort cash-flow visibility and make the loss harder to attribute.
UnitedHealthcare
UnitedHealthcare uses a mix of pre- and postpayment edits targeting high-level E/M visits, telehealth, and split or shared visits. The claims are flagged when they exceed payer-defined complexity or time thresholds and reassigned to lower levels pending appeal. UHC's broader use of AI in claims decisions has drawn legal scrutiny, including a court ruling indicating that AI tool use should be disclosed in coverage agreements.
The rest of the market
Automated downcoding is no longer a handful of payers. Per NBC News reporting and analyses from the American Society of Clinical Oncology and other groups, Aetna, Ambetter, Elevance (formerly Anthem), Blue Cross Blue Shield plans in multiple states, Humana, Kaiser, Molina, UnitedHealthcare, and Wellcare have all introduced coding-accuracy or payment-integrity programs that use algorithms to reduce E/M levels, often without reviewing clinical documentation.
Medicare Advantage downcoding: a distinct and growing front
Medicare Advantage deserves its own treatment, both because it operates under a different regulatory framework and because the compliance stakes for providers are higher.
MA plans apply the same basic mechanism as commercial payers - automated reduction of physician-submitted E/M codes from 99214 or 99215 to 99213 without individual clinical review - but two features make the MA situation distinct.
First, there is a clear regulatory standard to appeal against. The CMS 2024 Final Rule requires Medicare Advantage plans to apply coverage criteria consistent with traditional Medicare guidelines for coverage determinations. HHS OIG findings published in 2025 confirmed that several major MA plans were using AI tools to systematically deny and downcode claims without adequate clinical review. The OIG has placed MA plan oversight among its top priorities for 2025 and 2026, and CMS expanded its audit coder workforce dramatically (from roughly 40 to 2,000) as part of a more aggressive audit posture. That combination gives providers a documented, regulation-backed foundation for appeal that does not exist as cleanly on the commercial side: if your documentation satisfies the 2021 AMA E/M criteria for a 99214 and the MA plan paid a 99213, the appeal rests on the plan's own obligation to apply traditional-Medicare-consistent criteria.
Second, there is a False Claims Act dimension that cuts both ways. Passively accepting a downcoded MA payment is not neutral. When your documentation supports a 99215 but you accept a 99213 payment without appeal, a discrepancy exists between your clinical record and the encounter data the MA plan reports to CMS. In a federal audit, that gap can be characterized as reckless disregard of an incorrect payment. The practical implication: for Medicare Advantage in particular, appealing an unjustified downcode is not only about recovering revenue, it is about keeping your clinical record and the reported encounter data aligned.
A note on a related but separate MA issue to avoid confusion: much of the MA enforcement news concerns risk adjustment and HCC coding, where the alleged problem runs in the opposite direction (plans inflating diagnoses to raise risk scores and capture more CMS payment). That is a distinct enforcement area. The downcoding problem covered here is the one that reduces provider payment on E/M services. Both can be present in the same plan, but they are different mechanisms with different remedies.
It is also worth noting the broader MA access pressure: MA denial rates rose sharply (one analysis cited a 55.7% jump between 2022 and 2023), and some health systems have responded by reconsidering MA participation entirely. Downcoding sits inside this larger trend of automated payment suppression in the MA program.
The financial impact by specialty
Automated downcoding does not hit every specialty equally. The services most affected are the high-acuity, documentation-dependent encounters that legitimately qualify for Level 4 and Level 5 codes.
- Primary care and internal medicine. High volumes of 99214 and 99215 visits make even a small per-visit reduction add up quickly across a panel.
- Orthopedic surgery. Complex fractures, multi-comorbidity surgical planning, and high-risk implant procedures routinely justify Level 4 and Level 5 codes - exactly the codes algorithms are tuned to flag.
- Oncology. Complex, data-heavy visits integrating labs, imaging, and treatment planning are frequent downcoding targets, a concern raised directly by the American Society of Clinical Oncology.
- Emergency medicine. ED algorithms frequently downgrade Level 4 and Level 5 visits, citing insufficient linkage between the presenting problem, test interpretation, and medical decision-making.
- Sleep medicine. Sleep physicians integrate complex data (history, comorbidities, test results) in a single visit; downcoding minimizes that effort and can delay testing such as polysomnography.
- Cardiology. Beyond E/M, cardiology faces modifier and bundling-based downcoding when modifiers like 26 or TC are omitted or proprietary edits re-bundle professional and technical components.
- Inpatient services. DRG downgrades reclassify high-weighted DRGs (sepsis, acute respiratory failure) to lower groupings, reducing payment by $3,000 to $7,000 per claim.
The aggregate range cited across the industry is $40,000 to $180,000 per practice annually, with the position within that range driven by specialty, payer mix, and the share of legitimately high-acuity encounters.
How to detect automated downcoding
The detection challenge is structural: automated downcodes post as adjustments, not denials, so they are invisible to the reports most teams rely on. Surfacing them requires looking in the right places.
Run a submitted-code-versus-paid-code variance check. This is the single most important detection tool. It compares the code you billed against the code the payer actually paid, by payer. When the paid code is lower than the submitted code, you have a downcode. Most in-house teams do not run this check systematically, which is precisely why the problem stays hidden.
Read the remark and adjustment reason codes. Lines that look like routine explanations often signal an automated code change. Adjustment reason codes pointing to a code correction, "coding accuracy" review language, or payment that mathematically implies a lower-level code are all signals.
Watch the payment patterns. A payer whose denial rate is unchanged but whose average E/M payment is drifting downward is likely downcoding. Sudden reductions from a payer whose contract has not changed, payments that consistently land below your Medicare benchmark for commercial claims, and clusters of reduced payment on Level 4 and Level 5 codes all warrant a closer look.
Track by payer and by location. Because some programs are paused in some states (Cigna in California, for example) and active elsewhere, downcoding can vary across a multistate group. Tracking variance by payer and location surfaces these patterns.
The honest reality is that manual review catches only the obvious cases. The reliable approach is an automated variance engine that knows what each claim should have paid under the contract for the code that was billed, and flags every instance where the actual payment indicates a lower code was substituted.
How to appeal and recover
Once a downcode is identified, the appeal foundation is consistent across nearly every program.
Anchor the appeal in the 2021 AMA E/M guidelines. The guidelines define MDM levels using specific criteria: the number and complexity of problems addressed, the amount and complexity of data reviewed, and the risk of complications. If your documentation satisfies the criteria for the billed code, you have a defensible appeal. Submit the complete medical record and cite the specific criteria your documentation meets.
For Medicare Advantage, add the regulatory citation. Cite the CMS 2024 Final Rule requiring MA plans to apply criteria consistent with traditional Medicare, and reference the 2025 OIG findings. This gives the MA appeal a regulatory backbone the commercial appeal lacks.
Address the missing review directly. Because the downcode was applied without clinical review, the appeal can make that point explicitly: the payer reduced a documented code without examining the documentation that supports it.
Work the program-specific process. For Cigna prepayment downcodes, submit records and request reconsideration. For Aetna postpayment clawbacks, respond to the records request promptly and dispute the recoupment. For UnitedHealthcare, file for reconsideration with full documentation.
Prioritize and automate. Not every downcode is worth individual appeal, but systemic patterns are. Group appeals by payer and code, automate appeal-letter generation where possible, and track win rates by payer to focus effort where it pays off. The goal is to fix the trend, not just the single claim.
How to prevent it going forward
Recovery addresses claims already downcoded. Prevention reduces the volume and strengthens your position.
Strengthen documentation at the point of care. Capture full MDM detail - problem complexity, data reviewed, risk level - and record exact time for time-based codes rather than vague phrasing. Precise ICD-10 coding and explicit linkage between the presenting problem and the decision-making reduce the surface area an algorithm can exploit.
Educate providers and coders on payer-specific rules. Teams cannot defend against rules they do not know. Keep providers current on the Cigna, Aetna, and UnitedHealthcare programs and how each one behaves.
Benchmark your own coding distribution. Because many programs flag outliers against peer averages, knowing where your E/M distribution sits - and being able to justify it clinically - is a defensive asset. If your patient mix genuinely skews complex, document why.
Build the monitoring layer. The most durable prevention is continuous, automated variance detection that catches downcoding the moment it appears, by payer and by code, so trends get addressed before they compound across thousands of claims.
How MD Clarity helps
Automated downcoding is, at its core, a payment that does not match what the contract owed for the code that was billed - which is exactly the variance RevFind was built to detect.
RevFind digitizes the full contract portfolio and runs every remittance through a pricing engine that replicates payer adjudication at the charge-line level. Because it knows what each claim should have paid under the contract for the code you submitted, it flags the moment a payment indicates a lower code was substituted - the submitted-code-versus-paid-code variance that hides inside an adjustment and never reaches a denial report. RevFind surfaces these downcodes into prioritized worklists and trends them by payer, code, and location, so a multistate group can see exactly where Cigna, Aetna, UnitedHealthcare, or a Medicare Advantage plan is reducing payment and by how much.
For teams that need help pursuing what RevFind identifies, Underpayment Recovery Services supplies reimbursement specialists who build the documentation-anchored appeal, cite the applicable E/M and CMS standards, and pursue recovery through the payer's reconsideration and escalation channels. The combination turns automated downcoding from invisible, silent leakage into a tracked and recoverable revenue stream.
Get a demo to see RevFind flag a downcoded claim and trace it back to the contracted rate for the code you actually billed.
FAQs
What is payer downcoding?
Payer downcoding is when an insurer reduces a physician-submitted billing code to a lower-level, lower-paying code, cutting reimbursement even when the higher level of care was delivered and documented. Today it is overwhelmingly automated: payer algorithms read structured claim data, compare it against peer-coding benchmarks or a proprietary payment matrix, and reassign the code in seconds without reviewing the medical record. It most often targets high-level E/M codes such as 99214 and 99215, reducing them to 99213.
Which payers are downcoding claims automatically?
By 2026, more than ten major insurers run automated coding-accuracy or payment-integrity downcoding programs. The most prominent are Cigna (E/M Coding Accuracy, the R49 policy effective October 2025), Aetna (E/M Claim and Code Review Program), and UnitedHealthcare. Humana, Elevance, regional Blue Cross Blue Shield plans, Kaiser, Molina, Ambetter, and Wellcare have similar programs. Medicare Advantage plans across multiple carriers also apply automated E/M reductions.
Is automated downcoding legal?
Downcoding itself is not inherently illegal, but it can violate contract terms or regulatory standards when applied without clinical review. The American Medical Association opposes automatic, algorithm-driven downcoding without record review. For Medicare Advantage, the CMS 2024 Final Rule requires plans to apply coverage criteria consistent with traditional Medicare, and 2025 HHS OIG findings confirmed several MA plans were downcoding without adequate clinical review, which establishes a regulatory basis for appeal.
How much revenue does automated downcoding cost a practice?
Industry estimates place the cost at $40,000 to $180,000 annually for the average practice. Each downcoded E/M visit typically loses $45 to $80 (for example, 99214 reduced to 99213). Inpatient DRG downgrades can reduce payment by $3,000 to $7,000 per claim. The exact impact depends on specialty, payer mix, and the proportion of high-acuity encounters that legitimately qualify for Level 4 and Level 5 codes.
What is the difference between downcoding and a denial?
A denial is an explicit refusal to pay all or part of a claim, identified by a denial code on the remittance and visible on denial reports. A downcode is a paid claim where the payer reduced the code to a lower level, posted as a payment adjustment with no denial signal. Denials are tracked by most revenue cycle teams; downcodes are systematically missed unless a submitted-code-versus-paid-code variance check is run.
How do you appeal an automated downcode?
Appeal with the medical record and a citation to the 2021 AMA E/M guidelines showing that your documentation satisfies the medical decision-making or time criteria for the code you billed. For Medicare Advantage, also cite the CMS 2024 Final Rule requiring criteria consistent with traditional Medicare. Because the downcode was applied without clinical review, a documented record that supports the billed level is a strong basis for reversal.
Get paid in full by bringing clarity to your revenue cycle
Related Posts


Subscribe to the

Healthcare Clarified newsletter
Get the latest insights on RCM and healthcare policy in your inbox
