Hospital Underpayments: A Complete Guide to Detecting and Recovering Lost Revenue
.avif)
.svg)
.svg)
What Are Hospital Underpayments?
Hospital underpayments occur when a commercial or government payer reimburses a hospital less than the amount specified in its contracted rate, fee schedule, or applicable regulatory requirement. Unlike outright denials, underpayments are often partial payments that arrive without warning - the claim is "paid," but the dollar amount is short of what the contract entitles the hospital to receive.
Because each individual variance can be small, sometimes only tens or hundreds of dollars per claim, underpayments are easy to overlook. Across millions of claims a year, however, those small variances compound into substantial revenue leakage that erodes operating margins and limits the hospital's ability to invest in patient care.
This guide breaks down what causes hospital underpayments, how much they typically cost providers, how to identify and recover them, and how to prevent them from happening in the first place.
Why Hospital Underpayments Matter
Hospitals operate on famously thin margins. According to HFMA analysis, the aggregate operating margin among all U.S. hospitals sits around 5.2% post-pandemic, and 39% of hospitals were running at negative operating margins as recently as 2023. In that environment, even a modest underpayment rate can be the difference between profitability and red ink.
Underpayments hurt hospitals in three compounding ways:
- Direct revenue loss. Every dollar shorted on a claim is a dollar the hospital has already spent providing care but will never collect.
- Operational drag. Identifying and appealing underpayments requires skilled staff time, particularly when teams rely on manual spreadsheet reconciliation against complex payer contracts.
- Negotiation disadvantage. Without precise data on how each payer is actually performing against contract terms, hospitals enter renegotiations with anecdotes instead of evidence, and often accept terms that perpetuate the problem.
Top Causes of Hospital Underpayments
Most healthcare underpayments trace back to a handful of recurring root causes. Understanding which ones drive the most dollar loss at your organization is the first step toward systematic recovery.
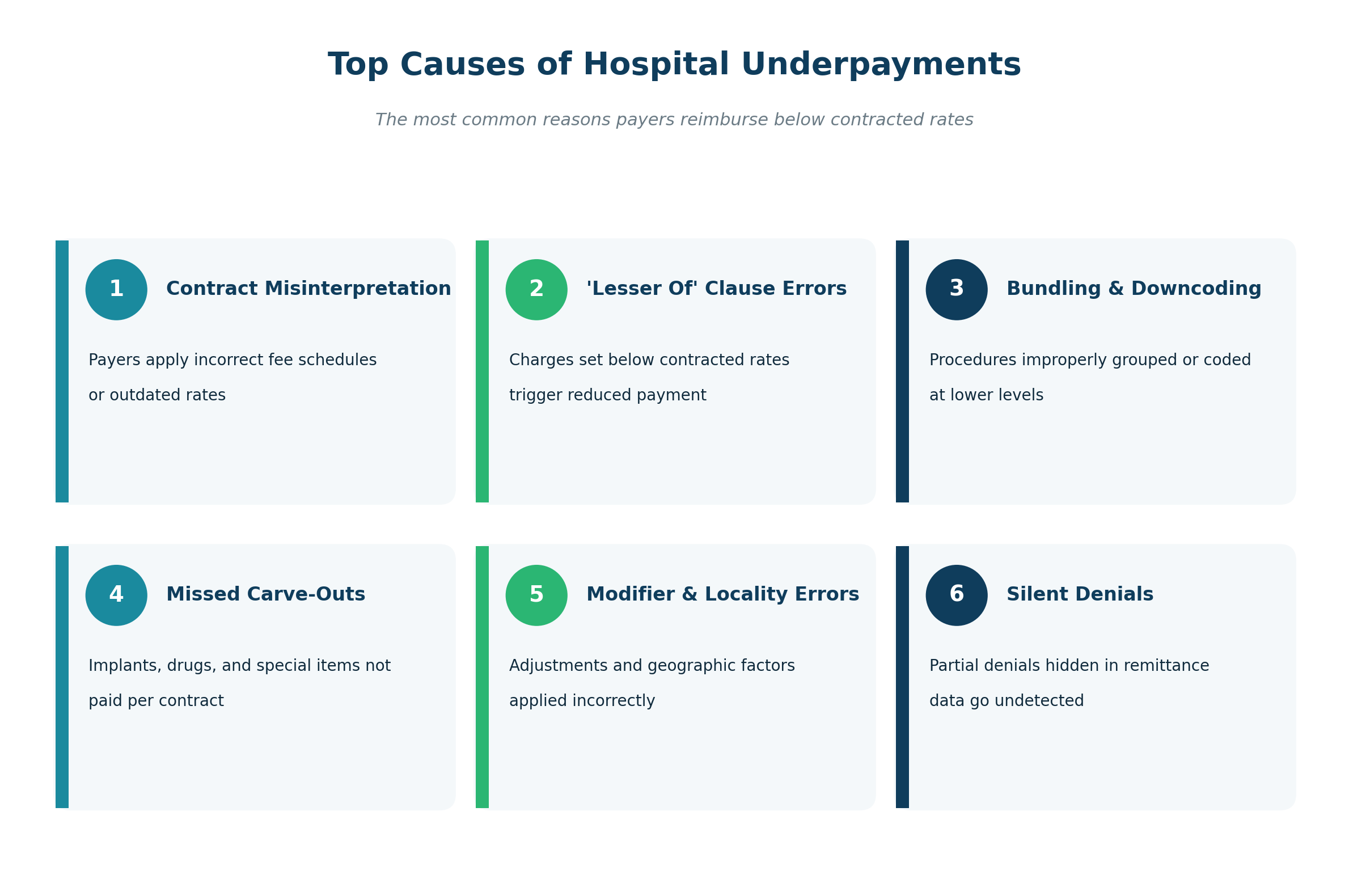
1. Contract Misinterpretation
Payer contracts are dense, multi-hundred-page documents with layered fee schedules, exceptions, and carve-outs. When a payer's adjudication system applies the wrong fee schedule version, an outdated rate table, or misreads a contract clause, the result is a chronic underpayment that may persist across thousands of claims before anyone notices. HFMA has begun calling this gap Policy Drift, the operational lag between when a payer changes a rule and when the change is reflected in provider workflows.
2. "Lesser Of" Clause Errors
Many hospital contracts include a "lesser of" provision: the payer will reimburse either the contracted rate or the hospital's billed charge, whichever is lower. If the chargemaster price for a service is set below the contracted rate, the hospital is effectively capping its own reimbursement. Identifying and correcting these chargemaster gaps is a major underpayment recovery lever.
3. Bundling and Downcoding
Payers sometimes bundle separately reimbursable procedures into a single code, or downcode a higher-level service to a lower-paying one. Both practices reduce reimbursement below what the contract specifies for the services actually rendered.
4. Missed Carve-Outs
Implants, high-cost drugs, blood products, and certain specialty services are often "carved out" of standard rates and reimbursed separately. When payers ignore carve-out provisions and bundle these items into a base rate, hospitals lose reimbursement that can range from hundreds to tens of thousands of dollars per case.
5. Modifier and Locality Errors
Anesthesia time units, multiple-procedure modifiers, and geographic locality adjustments all influence the correct payment amount. Small errors in how these are applied compound quickly across high claim volumes.
6. Silent Denials
A "silent denial" is a partial denial buried inside a remittance. The claim is reported as paid, but one or more line items have been zeroed out without an explicit denial code. These are particularly costly because they bypass standard denial workflows and often go undetected entirely.
Hospital Underpayments vs. Denials: What's the Difference?
A denial is a payer's explicit refusal to pay a claim or line item. An underpayment is a partial payment that falls short of the contracted amount, even though the claim was "accepted" and processed.
The two are related but require different workflows.
Denials show up on the remittance with an explicit denial code, making them visible to any standard claim denial rate report. They are typically owned by a denials management team, and recovery involves correcting and appealing the claim before resubmitting it to the payer.
Underpayments are hidden in the difference between what a claim should have paid under contract terms and what the payer actually remitted. They require contract-based variance modeling to detect, sit with the contract management or payment integrity team, and are recovered through variance disputes, payer escalation, and contract enforcement.
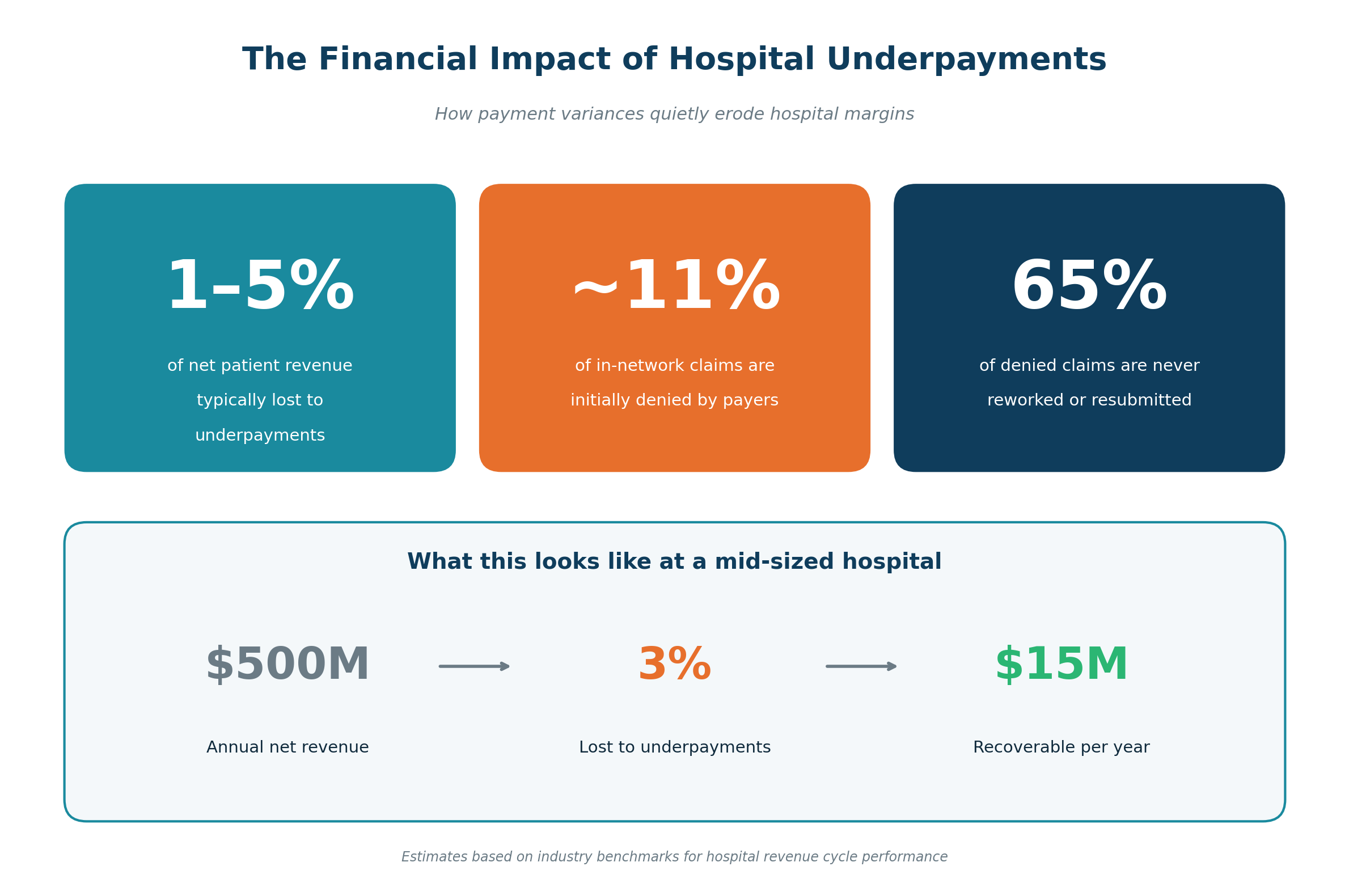
Hospitals that focus only on denials and not on underpayments routinely leave 1-3% of net revenue uncollected. A complete revenue integrity program addresses both.
The Financial Impact of Hospital Underpayments
According to HFMA benchmarks, hospitals are typically underpaid between 2% and 5% of net patient revenue. Broader revenue leakage estimates, which include missed charges, denials, and underpayments together, put the figure at 3-5% of net revenue annually, totaling tens of billions of dollars across the U.S. healthcare system. For a hospital with $500 million in annual net revenue, that translates to $15-25 million in recoverable revenue every year.
How to Detect Hospital Underpayments
Detecting underpayments at scale requires comparing what each claim was actually paid against what it should have been paid under the contract, at the charge level. That comparison can be done three ways:
1. Manual Spreadsheet Audits
Staff pull samples of paid claims, look up contract terms, and recalculate expected payment by hand. This approach is accurate for small samples but cannot scale to the millions of claims a typical hospital processes, and it surfaces only the variances staff happen to sample.
2. Payer-Provided Adjudication Reports
Some payers offer self-service explanations of how a claim was adjudicated. These reports are useful for investigating individual claims but rarely sufficient for systematic detection, because the payer is unlikely to flag its own underpayments.
3. Contract Modeling Software
Modern revenue integrity platforms replicate payer adjudication logic, including modifiers, locality adjustments, carve-outs, and "lesser of" rules, and apply it to every claim automatically. Any variance between modeled expected payment and actual payment becomes a flagged work item, no sampling required.
The third approach is the only one that scales. It is also the only one that catches silent denials and small per-claim variances that, individually, no human auditor would flag.
The Hospital Underpayment Recovery Workflow
A mature underpayment recovery program follows a repeatable five-step workflow:
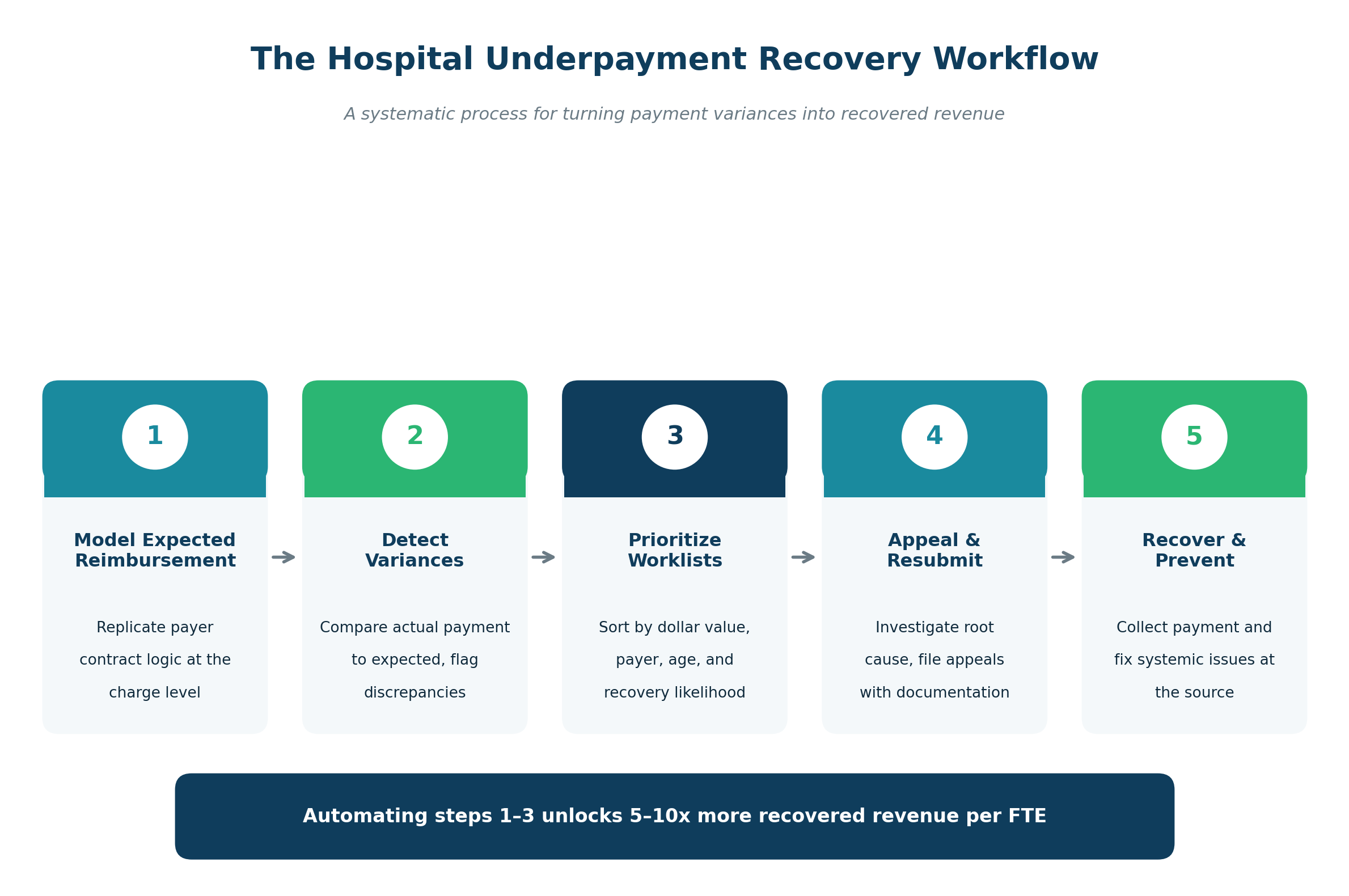
Step 1: Model Expected Reimbursement
Replicate each payer contract, including fee schedules, carve-outs, modifiers, and case-rate logic, so the system can calculate what every claim should have paid.
Step 2: Detect Variances
Compare actual remittance amounts against modeled expected amounts. Flag any claim where the difference exceeds a defined threshold.
Step 3: Prioritize Worklists
Not every variance is worth pursuing. Smart prioritization ranks work items by dollar value, payer responsiveness, claim age, and likelihood of successful appeal, so staff spend their time on the highest-yield cases first.
Step 4: Appeal and Resubmit
Investigate the root cause of each variance, gather supporting documentation (contract language, medical records, coding rationale), and file appeals with the payer. Dynamic status labeling and bulk export tools keep large appeal batches organized.
Step 5: Recover and Prevent
Collect recovered payment and, just as importantly, feed root-cause data back into the contract management and chargemaster processes so the same variance does not recur. Drill-down reporting by payer, procedure code, and denial reason makes this feedback loop possible.
Hospital Underpayment Prevention Strategies
Recovery is necessary but reactive. The highest-performing hospitals also invest in prevention:
- Centralize all payer contracts in a digital repository with searchable terms, notice periods, and renewal dates, so no contract silently rolls over on disadvantageous terms.
- Audit the chargemaster against contracted rates at least annually to eliminate "lesser of" exposure and ensure pricing aligns with reimbursement methodology.
- Use contract modeling during negotiation to forecast the financial impact of proposed rate changes before signing. Knowing that a 2% rate increase on one CPT family is worth more than a 5% increase on another is the kind of leverage that improves contract economics.
- Track payer performance over time. Benchmarking how each payer pays, including clean claim rate, average days to payment, and underpayment rate, turns renegotiation from a guessing game into a data-driven conversation.
- Build feedback loops between recovery and contracting. When a root cause is identified during appeal, the contracting team needs to know so it can be addressed at the next renewal.
How Technology Closes the Hospital Underpayment Gap
Detecting and recovering hospital underpayments at scale is fundamentally a data problem. Hospitals need to model thousands of contract terms against millions of charge-level data points, every day, with audit-grade precision. That is not a job for spreadsheets, and it is not a job manual review can keep up with.
MD Clarity's RevFind is a revenue optimization platform purpose-built to solve this problem. RevFind digitizes payer contracts, fee schedules, and carve-outs and replicates payer adjudication logic with charge-level precision, factoring in modifiers, locality adjustments, and contractual policies, so hospitals know exactly what each claim should have been paid.
RevFind helps hospitals close the underpayment gap in four ways:
- Maximize reimbursement yield. Systematically identify revenue opportunities from underpayments and denials across every payer and procedure code, without manual spreadsheet reconciliation.
- Negotiate with data-driven leverage. Model the real-time revenue impact of proposed contract changes, benchmark payer performance, and enter negotiations with comprehensive analytics on every term that matters.
- Enhance operational efficiency. Automated worklists, dynamic claim status labeling, and bulk exports streamline recovery workflows, while dashboards track resolution progress with full audit trails.
- Scale with confidence. Handle every reimbursement methodology, from straightforward fee-for-service to intricate anesthesia and case-rate calculations, across all facilities and data sources.
For hospitals that want full-service support, MD Clarity's Underpayment Recovery Services pairs RevFind's variance detection with expert payer reimbursement specialists who manage end-to-end claim resolution, fixing sources of revenue leakage while reducing internal staff workload.
Book a demo to see how RevFind can optimize your hospital's revenue.
Frequently Asked Questions
What is a hospital underpayment?
A hospital underpayment is a partial payment from a commercial or government payer that is less than the amount the hospital is contractually entitled to receive. Unlike a denial, the claim is processed and paid, just not in full, which is why underpayments often go undetected.
How much do hospital underpayments cost the industry?
Industry benchmarks estimate that hospitals lose 2-5% of net patient revenue to underpayments alone, and 3-5% to total revenue leakage including denials. For a $500 million hospital, that is $15-25 million in recoverable revenue per year.
How are hospital underpayments different from denials?
A denial is an explicit refusal to pay a claim or line item, with a denial code on the remittance. An underpayment is a partial payment that falls short of the contracted amount despite the claim being accepted. The two require different detection methods and workflow owners.
How long do hospitals have to appeal an underpayment?
It varies by payer and contract. Most commercial payer contracts specify a timely filing window for disputes ranging from 90 to 365 days from the date of remittance. Hospitals should track each payer's window in their contract management system to avoid forfeiting recoverable dollars.
Can hospitals recover underpayments from years ago?
In most cases, no. Payer contracts typically cap the look-back window at 12-24 months. This is one of the reasons systematic, automated detection matters: variances identified within the dispute window can be recovered, while older variances are usually written off.
What is the best way to prevent hospital underpayments?
The most effective prevention combines four practices: digitizing and centralizing payer contracts, auditing the chargemaster against contracted rates, modeling proposed contract terms before signing, and feeding root-cause data from recovery efforts back into contract negotiations.
What software is best for detecting hospital underpayments?
Look for a platform that models payer adjudication logic at the charge level, handles every reimbursement methodology (fee-for-service, case rate, anesthesia time units, percent of charges), centralizes contracts in a searchable repository, and produces audit-grade calculations with full charge-by-charge breakdowns. MD Clarity's RevFind is purpose-built for these requirements.
FAQs
Get paid in full by bringing clarity to your revenue cycle
Related Posts

Subscribe to the

Healthcare Clarified newsletter
Get the latest insights on RCM and healthcare policy in your inbox
