.avif)
.svg)
.svg)
Post-acquisition revenue cycle integration is the structured process of unifying billing, payer contracting, denial management, and patient collections across newly acquired physician practices into a single, standardized MSO operation. Done well, it protects the EBITDA that underwrote the acquisition. Done poorly, it quietly erodes 6 to 16 percent of net patient revenue every year through underpayments, denials, and patient bad debt that nobody is watching.
This playbook is for MSO CFOs, VPs of revenue cycle, VPs of managed care, and the private equity operating partners who back them. It covers what to do before close, on Day 1, in the first 90 days, and through the 180-day mark - and the KPIs that tell you whether integration is actually working.
What is post-acquisition revenue cycle integration?
Post-acquisition revenue cycle integration is the operational discipline of taking a newly acquired physician practice or group and folding its billing, payer contracts, denial workflows, patient financial experience, and reporting into the MSO's centralized revenue cycle operation. It spans both technology consolidation (EHRs, practice management systems, clearinghouses, contract management software) and process standardization (charge capture, claim scrubbing, denial appeals, patient estimates, collections).
The goal is not just to keep cash flowing through the closing period. The goal is to capture the back-office synergies that private equity sponsors and platform MSOs typically underwrite at 200 to 300 basis points of margin improvement within the first two years post-close.
Why post-acquisition revenue cycle integration matters more than ever
Three forces have made RCM integration the single highest-leverage activity in an MSO add-on acquisition.
First, deal volume is sustained. Private equity represents more than 90 percent of physician practice M&A transactions, and the pace of physician practice consolidation has held steady through 2025 and into 2026 despite broader market headwinds. The GAO has documented that non-hospital corporate owners, including PE firms and insurers, now exceed hospitals and health systems in physician practice ownership.
Second, payer behavior is getting worse, not better. Initial claim denial rates hit 11.8 percent in 2024, up from 10.2 percent a few years earlier, and 41 percent of providers now report denial rates above 10 percent. Nearly 88 percent of revenue cycle leaders surveyed by Guidehouse and HFMA say payer challenges are their top stressor. Every practice you acquire brings its own payer contract complexity, denial backlog, and underpayment exposure into your platform.
Third, synergies don't capture themselves. McKinsey's research across thousands of deals shows that cost synergies typically capture 70 to 85 percent of announced value while revenue synergies capture only 25 to 35 percent. BDO's CFO survey found that 35 percent of acquirers either missed or fell short of their synergy targets. The acquirers who track synergies from Day 1 outperform those who wait.
The hidden revenue leakage risks after a physician practice acquisition
Most acquired practices are leaking revenue in ways nobody on their team has the time, tools, or incentive to find. The dollars hide across six categories.
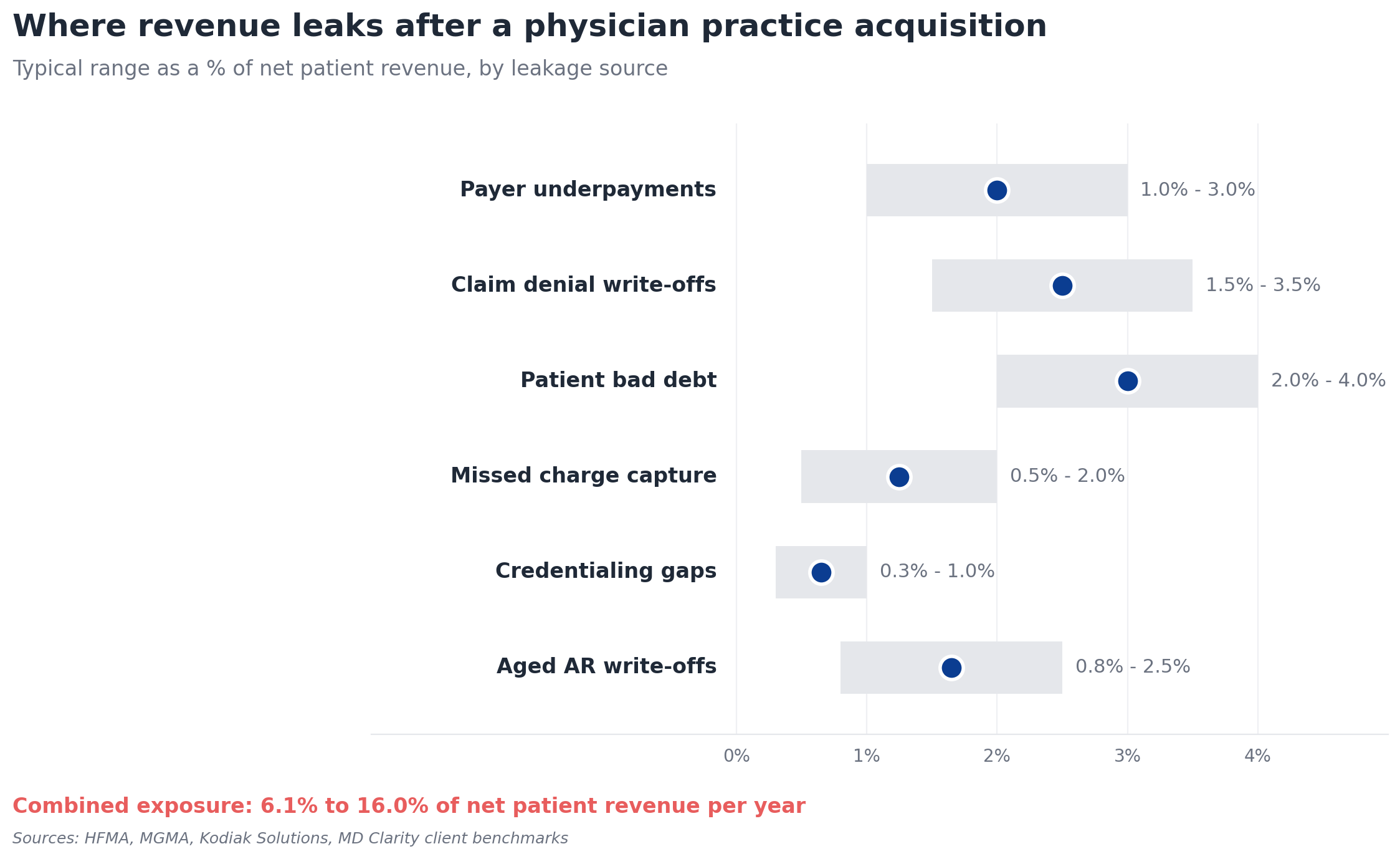
Payer underpayments
Payers routinely reimburse below contracted rates. Industry estimates put underpayments at 1 to 3 percent of net patient revenue annually for the average organization. Most acquired practices have never systematically compared remits against contracted rates at the CPT, modifier, and site-of-service level. The variance shows up as small dollars per claim that compound into millions across an MSO platform.
Claim denial write-offs
Initial denials are climbing, and many never get reworked. The cost to rework a single denied claim ranges from $25 to $181, and a significant share of denials become permanent write-offs because staff prioritize the current claim queue over older work.
Patient bad debt
With patient responsibility now making up roughly 30 percent of provider revenue, weak upfront collection processes hit the bottom line hard. The Kodiak Solutions benchmark shows patient collection rates fell to 47.8 percent in 2023, down from 54.8 percent in 2021. Acquired practices without automated patient estimates and pre-service collections typically have the worst exposure.
Missed charge capture
Charges that never make it onto a claim never get paid. Acquired practices with outdated charge capture workflows, weak EHR integration, or specialty-specific gaps (especially in procedural specialties) lose 0.5 to 2 percent of net patient revenue this way.
Credentialing gaps
When acquired providers aren't fully credentialed across the MSO's payer panel, claims are billed under the wrong TIN or denied outright. Industry-watchers benchmark credentialing leakage at roughly 0.3 to 1 percent of net revenue when providers' second six months underperform their first by more than 25 percent.
Aged A/R write-offs
A/R over 90 days carries a collection probability that drops below 65 percent past 120 days and below 41 percent past 180. Acquired practices commonly carry 28 to 35 percent of total A/R in the 90-plus bucket, well above the 18 to 22 percent benchmark.
The 4-phase post-acquisition revenue cycle integration framework
Integration runs cleanest as a sequenced 180-day program. Each phase has different objectives, different KPIs, and different risks. Skipping phases (especially Phase 1) is the most common reason synergies leak.
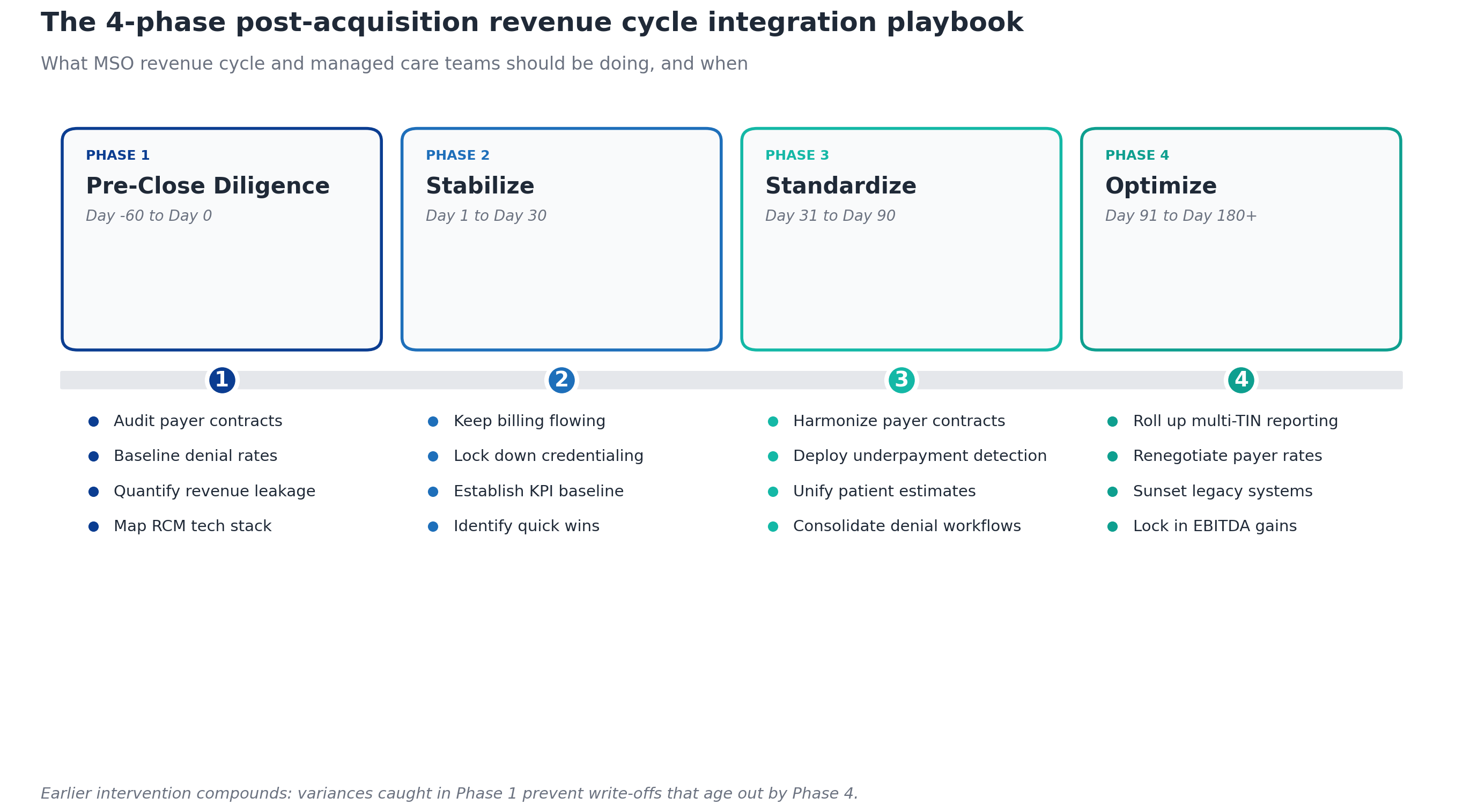
Phase 1: Pre-close revenue cycle due diligence (Day -60 to Day 0)
The single biggest predictor of integration success is whether revenue cycle leaders are involved in due diligence. McKinsey found that due diligence fails to provide an adequate roadmap for capturing synergies 42 percent of the time. For MSO add-on acquisitions, that gap is almost always in revenue cycle.
What to audit before close
The pre-close RCM diligence checklist covers four buckets:
- Payer contracts. Every commercial, Medicare Advantage, and Medicaid managed care contract should be loaded into a contract management platform with fee schedules at the CPT level. Identify expired, evergreen, and out-of-network arrangements.
- Denial baseline. Pull 12 to 24 months of remits and calculate first-pass denial rate by payer, by denial reason code, and by specialty. Anything above 7 percent suggests a process issue you'll inherit.
- Underpayment exposure. Sample 90 days of paid claims and compare them against contracted rates. A 1 percent variance on $50 million net patient revenue is $500,000 of recurring annual leakage you can model into the deal.
- Technology inventory. Map every EHR, practice management system, clearinghouse, denial management tool, and contract management platform in use. Note which are cloud, which are on-prem, and which have known data export limitations.
This is where third-party financial due diligence earns its fee. Independent diligence catches what target management can't see in their own data.
Red flags that warrant a price adjustment
Three findings should trigger a renegotiation conversation:
- First-pass denial rate above 12 percent (industry benchmark is 5 to 10 percent)
- A/R over 90 days exceeding 30 percent of total A/R
- More than 5 percent of paid claims showing variance against contract
Phase 2: Day 1 to Day 30 - stabilize
The first 30 days are about not breaking what works. Acquired practices have fragile workflows, and aggressive integration in the first weeks usually causes a cash collapse exactly when finance teams need stability.
Critical Day 1 actions
- Keep billing flowing under existing TINs and payer contracts. Do not migrate any claims to a new platform yet.
- Lock down credentialing. Verify every acquired provider is properly credentialed with every contracted payer under the correct TIN. Re-credentialing takes 90 to 120 days, so any gap surfaced here becomes a Phase 3 problem if you don't start now.
- Preserve patient communication channels. Patients expect continuity. Do not send rebranded statements or change patient portal access in Week 1.
- Establish a daily cash dashboard. Track cash posted by acquired entity for the first 60 days against the trailing 12-month average. Variances above 10 percent get same-day root-cause analysis.
Establish KPI baselines
Before you change anything, you need to know what "before" looked like. Calculate every KPI from the scorecard below for the acquired entity in isolation, using their last six months of data. These become your Day 0 baseline.
Identify quick wins
The most common quick win in Week 2 or 3 is loading the acquired entity's payer contracts into the MSO's contract management platform and running an underpayment scan against the trailing 90 days of remits. Recovered underpayments fund the rest of integration. One orthopedics MSO using this approach found $10.3 million in underpayments across their platform, with Community Care Partners recovering $160,000 from a single CPT code within three months.
Phase 3: Day 31 to Day 90 - standardize
Phase 3 is where the synergies actually start landing. The objective is to bring acquired practices onto MSO-standard workflows, contracts, and technology.
Harmonize payer contracts
Acquired practices almost always have weaker payer rates than the MSO platform - that's part of why the MSO is acquiring them. But harmonization is not automatic. Most commercial payer contracts have anti-assignment clauses, change-of-control notice requirements, and rate provisions that don't auto-extend. The managed care team should:
- Notify payers of the change of control per contractual requirements
- Identify which acquired contracts can be terminated and rolled onto the MSO master contract
- Identify which need to remain in place until renewal
- Build a renegotiation queue ranked by revenue impact
The opportunity is real. PE-backed MSOs use scale to negotiate higher reimbursement rates through consolidated bargaining power.
Deploy underpayment detection across all TINs
Acquired practices typically have no underpayment detection in place. Loading their contracts into a platform like MD Clarity's RevFind alongside the MSO's existing contracts lets the same engine detect variances on every TIN in the platform. This is where the multi-TIN reporting advantage compounds. You can see which payer is underpaying which specialty in which geography, and route recovery work to the right team.
Unify the patient financial experience
If the MSO is sending automated Good Faith Estimates and collecting deposits upfront, but the acquired practice is still hand-typing estimates into spreadsheets, the patient experience is inconsistent and so is cash performance. Standardizing on a single patient estimate software across all entities is one of the highest-ROI Phase 3 moves, because it both lifts upfront collections and reduces the bad debt that compounds in Phase 4.
Consolidate denial workflows
Most acquired practices manage denials reactively. The MSO standard should be:
- Root-cause categorization on every denial (eligibility, authorization, coding, medical necessity, contract)
- A central queue routed by payer and denial type rather than by acquired entity
- Appeals tracking with success-rate measurement by appeal type
Phase 4: Day 91 to Day 180+ - optimize
By Phase 4, the acquired practice should be operating on MSO-standard processes. Now the work shifts from integration to optimization.
Roll up multi-TIN reporting
The CFO and PE board want to see the full platform consolidated. That requires:
- Net revenue and EBITDA by TIN, specialty, site, and provider
- Payer mix and yield comparisons across acquired and legacy entities
- Variance analysis showing where each acquired practice has converged toward MSO benchmarks
Renegotiate payer rates with platform leverage
With contracts harmonized and performance baselined, the managed care team can now go back to payers with platform-level data. Higher patient volumes, broader geographic reach, and value-based care readiness all support rate increase requests.
Sunset legacy systems
Most MSOs accumulate three to seven practice management systems through serial acquisitions. Phase 4 is when the integration team retires the redundant ones - usually by migrating the acquired practice's historical data into the MSO master system and decommissioning the legacy environment. The savings are real: IT integration delays are one of the most common reasons synergies fail to land.
Lock in EBITDA gains
The final Phase 4 deliverable is a documented synergy realization report that ties measured RCM improvements - higher net collection rate, lower denial rate, recovered underpayments, faster A/R - back to the pre-close synergy thesis. This is what supports the next add-on acquisition and the next round of platform financing.
The KPIs every MSO should track during integration
You can't manage what you don't measure. These eight KPIs form the standard MSO integration scorecard. Baseline them at Day 1 for the acquired entity, track them weekly through Phase 2, monthly thereafter, and compare them against MSO platform averages.
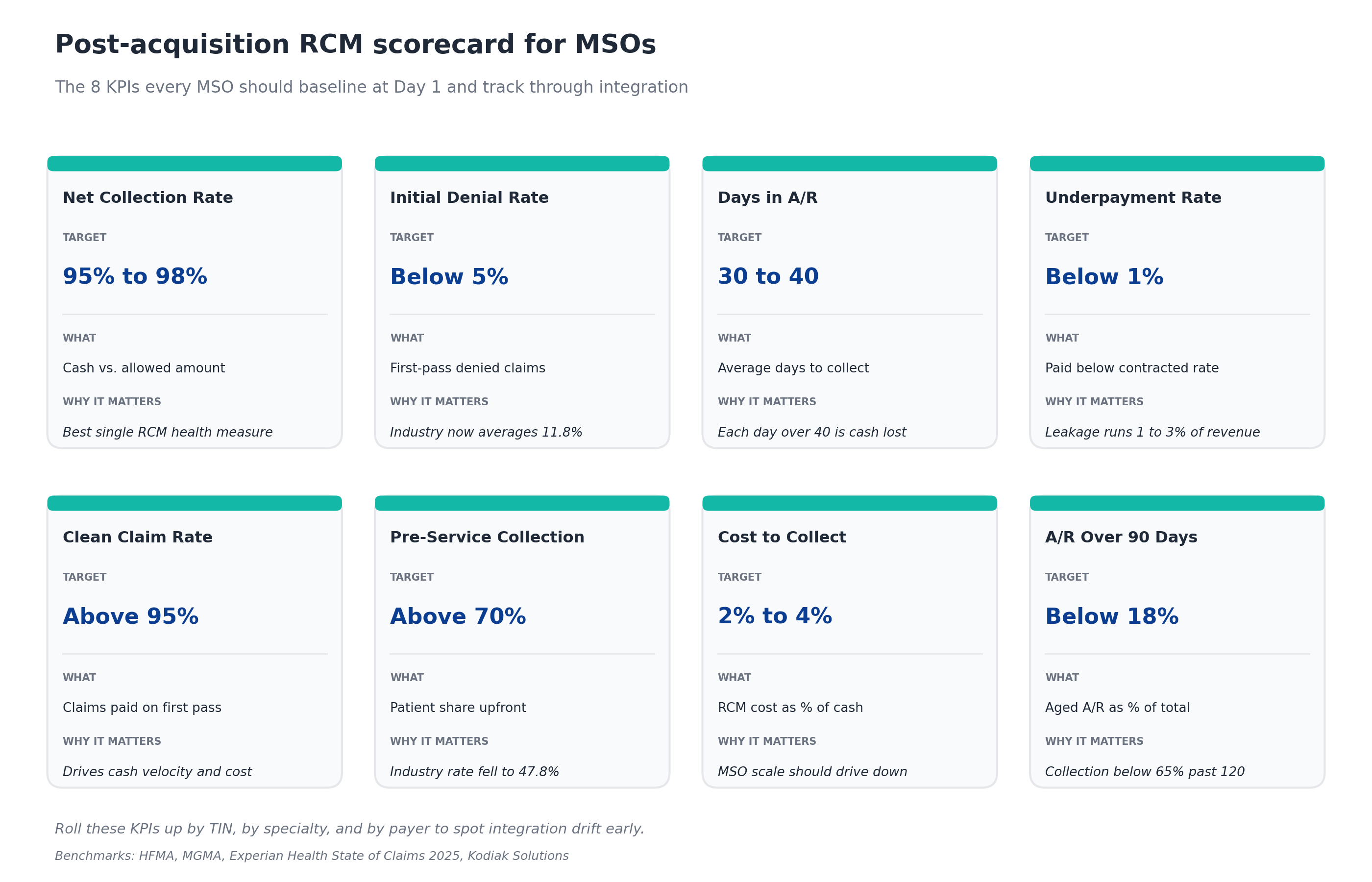
The discipline that separates successful integrations from struggling ones is rolling these KPIs up by TIN, by specialty, and by payer. Aggregate platform numbers hide the acquired practice that's been silently dragging on cash for six months.
Common post-acquisition revenue cycle integration mistakes
After watching dozens of MSO platforms run this play, five mistakes show up over and over.
Skipping Phase 1. Revenue cycle leaders learn about the deal the day it closes. By then the synergy assumptions are locked, the diligence questions are unanswered, and the acquired entity's problems become the MSO's problems without compensating price adjustments.
Migrating systems too fast. Forcing the acquired practice onto the MSO's EHR or practice management system in Phase 2 reliably crashes cash collections. Wait until Phase 4 unless there's a compliance reason to move sooner.
Ignoring credentialing. A provider billing under the wrong TIN generates denied claims that age into write-offs. Credentialing has to be Phase 2, not Phase 4.
Not loading the acquired contracts. If the acquired practice's payer contracts never get loaded into an MSO-wide contract management and underpayment detection platform, the leakage continues invisibly. You'll see the dollars in the next quarterly P&L review, not the variance report.
Treating integration as a project, not an operating model. The acquisitions don't stop. The next one is already in diligence. Integration capability is a permanent capacity, not a one-time effort.
How technology accelerates post-acquisition revenue cycle integration
Integration that depends entirely on manual processes (spreadsheets, ad hoc reports, individual analysts hand-checking variances) doesn't scale past two or three acquisitions. Most MSO platforms stand up three categories of technology to make integration repeatable.
Contract management and underpayment detection. A platform like RevFind centralizes every payer contract across every TIN, runs continuous variance detection against contracted rates, and routes recovery work to the right team. It also benchmarks rates and models payer negotiation scenarios at the platform level. This is the single highest-leverage technology investment for a multi-entity MSO, and the reason MD Clarity is consistently positioned as a leader in underpayment detection.
Patient estimation and pre-service collection. A platform like Clarity Flow automates Good Faith Estimate generation across all entities, sends estimates by text or email, and accepts upfront deposits - turning a manual spreadsheet workflow into a standardized patient experience and a more predictable cash forecast.
Multi-TIN denial and analytics. Denial management and reporting platforms that can aggregate across TINs, specialties, and payers let the central revenue cycle team see the platform as one operation rather than a stack of separate practices.
For a deeper look at how these three categories work together, MD Clarity's guide to revenue integrity walks through the operating model in more detail.
Frequently asked questions about post-acquisition revenue cycle integration
How long does post-acquisition revenue cycle integration take?
Most MSO add-on acquisitions complete core RCM integration in 90 to 180 days, with technology consolidation extending to 12 to 18 months. The four-phase framework above maps to a 180-day cycle for operational integration, with full platform rationalization (sunset of redundant systems, full payer contract harmonization) typically wrapping in year two.
What is the biggest risk in post-acquisition revenue cycle integration?
Cash disruption in the first 30 days is the highest-impact risk. Forcing system migrations, rebranded patient communications, or new claim submission processes in Phase 2 reliably suppresses collections for 60 to 90 days. The single best mitigation is keeping the acquired practice operating in its existing environment for the first month while baselining KPIs and identifying quick wins.
How do MSOs handle payer contracts after acquiring a practice?
Payer contracts cannot simply be transferred to the MSO. Most commercial contracts contain anti-assignment clauses requiring payer consent on change of control. The standard playbook involves notifying payers per contractual requirements, identifying which acquired contracts can be terminated and rolled onto the MSO master contract, and ranking the rest by renegotiation priority based on revenue impact and renewal date.
What KPIs matter most during integration?
The four KPIs that flag integration problems fastest are daily cash posted (compared to trailing 12-month baseline), first-pass denial rate, days in A/R, and underpayment rate against contracted rates. These four detect cash disruption, payer issues, billing issues, and contract issues respectively. The full eight-KPI scorecard above covers the rest.
How much revenue leakage is typical at an acquired practice?
Combined exposure across underpayments, denials, patient bad debt, missed charge capture, credentialing gaps, and aged A/R write-offs typically runs 6 to 16 percent of net patient revenue per year. For a $50 million net patient revenue practice, that's $3 million to $8 million annually - usually invisible until someone looks for it.
Can software replace the integration team?
No. Technology accelerates and scales the integration work, but the operating decisions (which contracts to terminate, which providers to credential first, which denials to appeal, when to migrate systems) require revenue cycle and managed care expertise. The right model is a small, repeatable integration team supported by a contract management and underpayment detection platform that handles the volume.
What does a successful integration look like at the 180-day mark?
A successful 180-day integration shows the acquired entity converged toward MSO benchmarks on net collection rate (within 2 points), denial rate (within 1 point), and days in A/R (within 5 days). Underpayments recovered during integration typically cover integration costs. Payer contract harmonization is in motion if not complete. And the integration team is already running the diligence checklist on the next add-on.
Build integration into the operating model
The MSOs that win this decade will not be the ones that close the most deals. They will be the ones whose post-acquisition revenue cycle integration capability is a repeatable, technology-enabled operating discipline rather than a heroic project run by exhausted analysts.
That means treating integration as a continuous capability, baselining every acquired entity against a standard KPI scorecard, and using contract management and underpayment detection software to make multi-TIN visibility automatic rather than aspirational.
MD Clarity helps MSO revenue cycle and managed care teams capture the underpayments, harmonize the payer contracts, and standardize the patient financial experience that determine whether an acquisition's EBITDA thesis actually lands. See the platform in action or read the orthopedics MSO case study for a real integration walkthrough.
FAQs
Get paid in full by bringing clarity to your revenue cycle
Related Posts


Subscribe to the

Healthcare Clarified newsletter
Get the latest insights on RCM and healthcare policy in your inbox
