Live Claims Monitoring: A Provider's Guide to Real-Time Underpayment Detection
.avif)
.svg)
.svg)
How real-time variance detection works, why it matters more as timely filing windows shrink, and what to look for when choosing a system.
Live claims monitoring is the continuous, real-time evaluation of payer remittances against contracted rates as ERAs are posted. Instead of waiting for a monthly batch or a quarterly audit to surface an underpayment, live monitoring flags the variance within hours of the remittance landing. The reason that timing matters: appeal timely-filing windows are short and shrinking, and the longer it takes to detect a variance, the smaller the runway to recover it.
Key takeaways
- Live claims monitoring evaluates remittances in real time. Detection happens within hours of the ERA posting, not weeks or months after the fact.
- Appeal windows are tighter than most teams realize. UnitedHealthcare commercial allows just 65 days, Medicare Advantage 60 days. Aetna, BCBS, Cigna, and Humana give 180.
- Manual and batch detection routinely miss the UHC window. Quarterly audits often surface a UHC underpayment after the appeal deadline has already closed.
- A complete system has six components. Contract repository, real-time claims feed, variance engine, smart prioritization, appeals workflow, and root-cause analytics.
- Software vs. service is a capacity question, not a capability one. Both paths can deliver live monitoring; the right one depends on whether you have the contract and managed-care specialists to run the workflow in-house.
What is live claims monitoring?
In healthcare revenue cycle, an underpayment is a claim that paid - but paid at less than the contracted rate. The remittance comes through, the claim closes in the patient accounting system, and the shortfall hides in the gap between the contracted amount and the deposited amount.
Live claims monitoring is the workflow that catches those shortfalls in real time. As each ERA posts, the system replicates payer adjudication logic, computes the expected reimbursement for every claim line, compares it against what the payer actually paid, and flags any variance that exceeds a defined threshold. The flag becomes a prioritized work item for the recovery team, complete with the contract citation needed to file an appeal.
The term "live" matters because it distinguishes the approach from two older methods:
- Manual review relies on staff cross-checking EOBs against contract terms, usually on a sample basis and usually weeks or months after payment. It catches obvious errors but misses systematic patterns and routinely runs past timely filing.
- Batch reconciliation runs variance reports on a scheduled cycle, typically monthly or quarterly. Detection is better than manual, but the 30-to-90-day lag still consumes a meaningful chunk of the appeal window.
Live monitoring closes both gaps. By detecting variances as remittances post, it preserves the full appeal window for every payer, including the ones with the shortest deadlines.
Why the deadline window is the whole game
The strongest argument for live monitoring is structural: payer appeal deadlines are short, vary widely by payer, and are strictly enforced. Miss the window by one day and the underpayment becomes permanent revenue loss with no review of the merits.
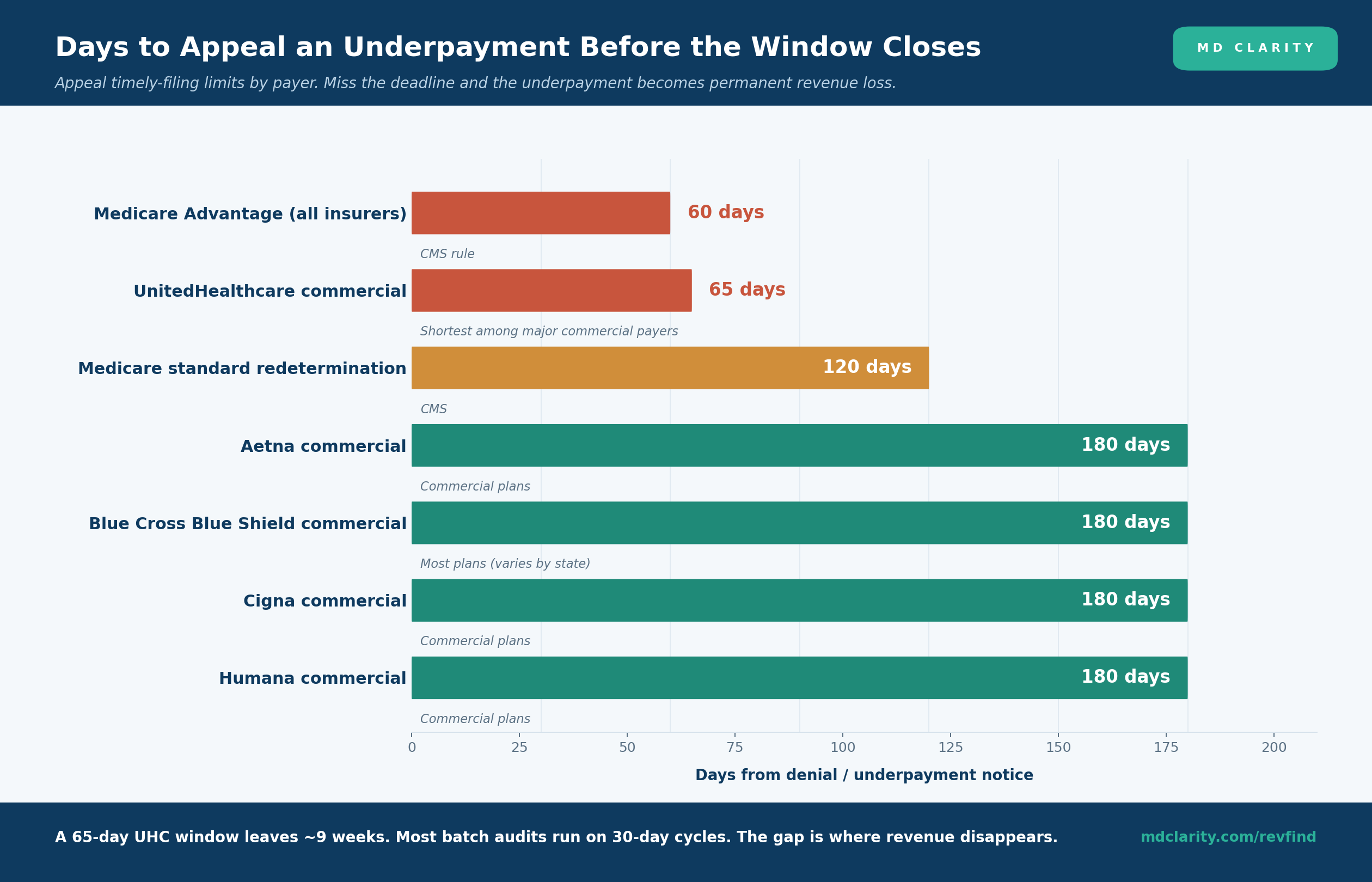
According to the 2026 payer-by-payer guide from Muni Health, UnitedHealthcare commercial plans require appeals within 65 calendar days of the denial or underpayment notice - less than half the window allowed by Aetna, Blue Cross Blue Shield, Cigna, or Humana, which all allow 180 days. All Medicare Advantage plans, regardless of the administering insurer, are bound by a 60-day CMS rule. Medicare standard redetermination allows 120 days.
These numbers reshape what "good" detection looks like. A team that catches underpayments through a monthly batch run loses 30 days of runway before the work item even surfaces. A team that audits quarterly is past UHC's deadline before the audit starts. As Medibill RCM reports, 84% of late appeals are unsuccessful unless supported by hard evidence of payer error - and an internal oversight delay does not qualify as an exception.
This is why "live" isn't a marketing adjective. It is a structural requirement to recover anything at all from the shortest-window payers.
Manual vs. batch vs. live: a timeline comparison
The clearest way to see the difference between detection approaches is to look at how each one consumes the appeal window.
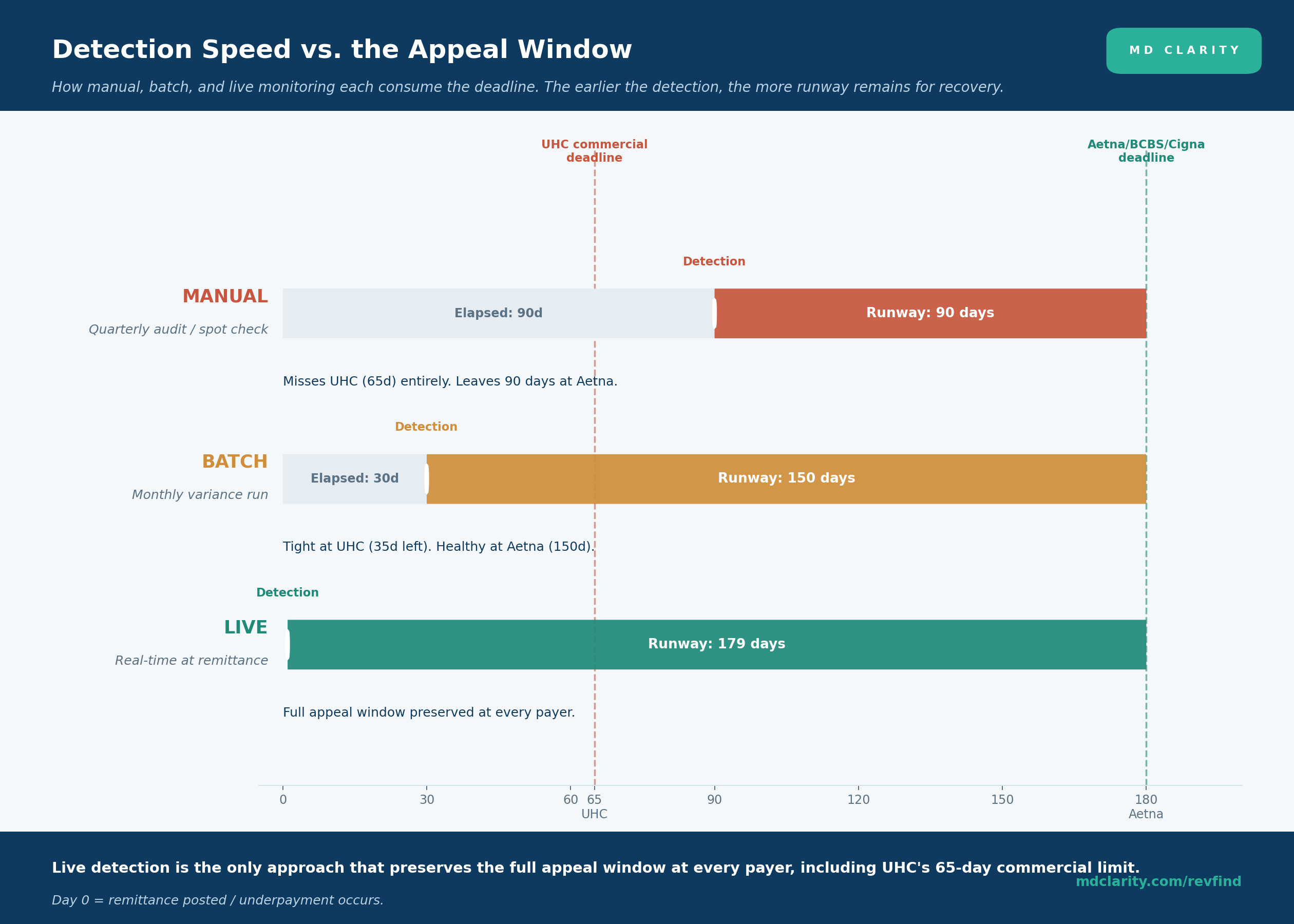
- Manual (quarterly audit). Detection lands around day 90. That leaves 90 days at Aetna or Cigna - workable - but is already 25 days past UHC's commercial deadline. Any UHC commercial underpayment surfaced this way is unappealable on its face.
- Batch (monthly variance run). Detection lands around day 30. That leaves a comfortable 150 days at the 180-day payers but only 35 days at UHC. The runway is tight, especially once internal review, packet assembly, and submission steps consume their own time.
- Live (real-time at remittance). Detection lands within hours of the ERA posting. The team has the full appeal window at every payer, with time for proper documentation and escalation.
For organizations that have meaningful UHC volume, the difference between batch and live is not stylistic. It is the difference between recovering most of the UHC variance and recovering very little of it.
Anatomy of a live claims monitoring system
A live monitoring platform that actually delivers on the promise has six distinct components. Missing any one of them means missed underpayments, missed deadlines, or both.

1. Contract repository. A complete, digitized record of every executed payer agreement, including fee schedules, carve-outs, modifiers, locality adjustments, case rates, stop-loss thresholds, and lesser-of clauses. The repository has to stay in sync as terms change or the variance engine starts producing false positives.
2. Real-time claims feed. Direct integration with your clearinghouse, practice management system, or data warehouse so that ERA/835 remittances are evaluated when payment posts. A nightly file drop is not a real-time feed.
3. Variance engine. The computational core. It must replicate payer adjudication logic at the charge-line level - not the claim level - because bundling errors, modifier issues, and partial-line underpayments are invisible at higher aggregation. The engine produces an expected-paid amount for every line, compares it to actual, and emits a variance whenever the gap exceeds a defined dollar or percentage threshold.
4. Smart prioritization. Not every variance is worth working. The system needs to rank flagged claims by dollar value, payer responsiveness, claim age relative to the timely-filing limit, and historical appeal win rate, so staff time goes to the recoverable dollars first.
5. Appeals workflow. Identifying variances is half the job. The system should generate payer-specific appeal packets that include claim identifiers, the variance math (expected vs. actual allowed), and the exact contract clause that supports the dispute. Tracking through escalation - secondary review, provider relations, legal - belongs in the same workflow.
6. Root-cause analytics. The prevention layer. Dashboards that trend variances by payer, code, modifier, and reason so contract managers, coders, and chargemaster owners can fix systematic causes. A recurring underpayment pattern on a single payer is worth more than any one-off appeal.
Common underpayment patterns live monitoring catches first
Live monitoring's structural advantage shows up most clearly on the categories of healthcare underpayment that batch and manual approaches struggle with. The recurring patterns:
- Incorrect fee schedule loads. When a payer's adjudication system is configured with last year's rates, every claim for the affected services underpays. Live monitoring catches the first instance; batch catches it weeks of leakage later.
- Modifier stripping. Modifiers 25, 59, and others that increase reimbursement get suppressed in payer processing without notification. Each instance is small; the cumulative dollar impact is significant.
- Improper bundling. Payers bundle services that the contract allows to bill separately, typically E&M services with same-day procedures. Detection at the charge line is the only way to see it.
- Silent partial payments. No remark code, no denial signal - just a remittance that paid less than the contract specifies. By definition, only contract-based variance detection catches these.
- Downcoding. The payer reimburses at a lower-level code than billed, often without notification. Live monitoring flags the mismatch immediately so coding teams can review documentation and appeal.
Each of these is recoverable when caught inside the appeal window. The recovery rate falls off a cliff after the deadline closes.
What to look for when evaluating live claims monitoring
Beyond the six core capabilities, a few requirements separate enterprise-grade live monitoring from feature-list software that struggles in production:
- Charge-line precision, not claim-level approximation. Anything less misses the systematic underpayment patterns where the dollars actually live.
- Native Medicare and commercial rules maintenance. The vendor should keep CMS fee schedules, locality adjustments, and similar reference rates current as part of the platform, not as a customer-managed configuration burden.
- Self-service contract loading and full-service onboarding. Both paths are useful; the first lets your team make changes on the fly, the second gets a large contract portfolio digitized fast.
- Multi-facility, multi-source data ingestion. Most provider organizations have more than one PM system and more than one clearinghouse. The monitoring platform needs to handle them without spreadsheet bridges.
- A complete audit trail. Every variance calculation should be traceable from the remittance line back through the contract clause and rate exhibit that produced the expected amount. Without that, appeals are unwinnable.
- Reporting that supports negotiation. Variance data is leverage at the contract table. The platform should make it easy to produce payer-level reports for negotiation cycles.
Build vs. buy vs. partner
Building a contract-modeling engine that mirrors payer adjudication is a multi-year engineering project with permanent maintenance overhead as fee schedules, modifiers, and policies change. Almost no provider organization gets a return on that investment versus buying.
The real choice is between purpose-built software (your team operates it) and a full-service partner (specialists operate it for you). A useful frame:
- Software-only. The right path for providers with experienced contract management staff and managed-care leadership who want operational control and want to retain institutional knowledge in-house.
- Full-service partner. The right path for providers with a meaningful underpayment backlog, limited specialist headcount, or complex commercial payer mixes. Faster ROI because specialists handle detection, appeals, and escalation end to end.
- Hybrid. Increasingly common - software for steady-state work, with a service partner for backlog clearance or high-complexity payers.
How MD Clarity supports both paths
MD Clarity's platform is built around the workflow above and gives you two ways to put it to work.
RevFind is the revenue optimization software. Use it to ingest claims and remittances in real time, replicate payer adjudication with charge-line precision, surface underpayments and denials into prioritized worklists, and digitize the full contract portfolio for ongoing variance detection and modeling.
Underpayment Recovery Services is the RevFind-enabled service. Specialists monitor every flagged variance, assemble contract-anchored appeals, and pursue each case through escalation, so you get recovered cash without adding headcount.
FAQs
What is live claims monitoring?
Live claims monitoring is the continuous, real-time evaluation of payer remittances against contracted rates as ERAs are posted. It flags underpayments within hours of the remittance landing rather than weeks or months later, preserving the full appeal timely-filing window for recovery.
How is live claims monitoring different from batch reconciliation?
Batch reconciliation processes claims in scheduled cycles, typically monthly or quarterly, so detection lags 30 to 90 days behind the remittance. Live claims monitoring evaluates every remittance as it posts, surfacing variances within hours. For payers with short appeal windows like UnitedHealthcare's 65-day commercial deadline, that lag is the difference between recovery and permanent revenue loss.
How long do you have to appeal an underpayment?
It depends on the payer. UnitedHealthcare commercial allows 65 calendar days. Medicare Advantage allows 60 days under CMS rules, regardless of which insurer administers the plan. Medicare standard redetermination allows 120 days. Aetna, BCBS, Cigna, and Humana commercial plans typically allow 180 days. Missing the deadline almost always results in automatic rejection without review of the merits.
What capabilities does a live claims monitoring system need?
Six: a digitized contract repository with current fee schedules, a real-time ERA/835 claims feed, a variance engine that replicates payer adjudication at the charge-line level, smart prioritization by dollar value and appeal-deadline urgency, an integrated appeals workflow with contract-anchored evidence, and root-cause analytics that prevent repeat leakage.
Does live claims monitoring replace denial management?
No. Denial management addresses claims that were explicitly rejected with a denial code on the remittance. Live claims monitoring addresses claims that were paid but underpaid relative to the contract - a separate problem with separate root causes. Mature revenue integrity programs run both workflows in parallel.
Should we build live claims monitoring in-house or buy it?
Buy. Building a contract-modeling engine that mirrors payer adjudication across every fee schedule, modifier, locality adjustment, and case rate is a multi-year engineering project with ongoing maintenance as payer rules change. Purpose-built software or a full-service partner gets to recovered cash in weeks rather than years.
Get paid in full by bringing clarity to your revenue cycle
Related Posts
.png)
Subscribe to the

Healthcare Clarified newsletter
Get the latest insights on RCM and healthcare policy in your inbox
