.avif)
.svg)
.svg)
A practical guide for hospitals, health systems, and physician groups to systematically recover the gap between contracted rates and what payers actually paid - and stop the leak at its source.
Underpayment collections is the process of identifying, appealing, and recovering the dollar gap between what a payer contractually owed for a healthcare claim and what the payer actually remitted. Unlike denials, underpayments arrive as partial payments without an outright rejection, which is exactly why they go unnoticed - and why most hospitals leave 1% to 3% of net revenue on the table every year.
Key takeaways
- Underpayments differ from denials. They are partially paid claims, invisible on standard denial reports, and only detectable through contract-based variance modeling.
- The financial stakes are large. Industry benchmarks place commercial-payer underpayments at 1% to 3% of net patient revenue - $5M to $25M annually for a $500M system.
- Recovery follows a 5-step process: Model the contract, detect variances, prioritize the work, appeal with contract-anchored evidence, and prevent recurrence.
- Appeals win on specificity. Citing exact contract language and rate exhibits beats generic complaints. Mature programs hit appeal win rates above 70%.
- Software, services, or both. Providers with mature managed-care teams can run collections in-house with purpose-built software; backlogged or under-resourced teams get faster ROI from a technology-enabled service partner.
What is "underpayment collections," exactly?
In healthcare finance, an underpayment occurs when a payer remits less than the rate specified in its contract with the provider. The remittance comes through, the claim closes in the patient accounting system, and on the surface everything looks fine. The shortfall is buried in the difference between what the contract entitled the provider to and what actually landed in the bank account.
Underpayment collections (sometimes called underpayment recovery or payment variance recovery) is the disciplined workflow that finds those shortfalls, builds a contract-anchored case to recover them, and closes the root causes so the same leakage doesn't repeat next quarter.
It is distinct from denial management, distinct from missed-charge recovery, and it requires a different toolset - one that can replicate every payer's adjudication logic claim-by-claim. As AGS Health notes, underpayments are a "hidden threat" precisely because most denial-focused teams never see them.
The financial stakes
Healthcare underpayments are not a rounding error. The numbers are well-documented across industry benchmarks and government data:
- 1-3% of net patient revenue is lost to commercial-payer underpayments annually
- $130 billion underpaid to U.S. hospitals by Medicare and Medicaid in 2023
- 83 cents on the dollar - what Medicare paid hospitals per dollar of care in 2023
- $43 billion spent by hospitals in 2025 chasing payments insurers owed
The American Hospital Association's Cost of Caring report documents that Medicare and Medicaid underpaid hospitals by $130 billion in 2023, with the gap growing roughly 14% annually since 2019. Becker's Hospital Review reports that hospitals received just 83 cents from Medicare for every dollar they spent on care that year.
On the commercial side, the leakage is harder to see but no less real. Most industry benchmarks - including those compiled by the Healthcare Financial Management Association - put commercial-payer underpayments at 1% to 3% of net patient revenue, with some estimates running as high as 5% for organizations with payer-heavy mixes or weak contract enforcement. For a $500 million health system, even the low end of that range is $5 million in recoverable cash sitting in aged A/R right now.
Underpayments vs. denials: why the distinction matters
If your revenue cycle team is focused exclusively on denial management, you are almost certainly missing the underpayment problem. They share a goal - getting paid what you're owed - but they behave very differently and require different tools.
- How the payer signals it. Denials arrive with an explicit denial code on the remittance. Underpayments come through as partial payments with no denial code - no signal at all.
- How you detect it. Denials show up on standard denial rate reports. Underpayments only surface through contract-based variance modeling against expected reimbursement.
- Who owns it. Denials sit with the denials management team. Underpayments belong to the contract management or payment integrity team.
- How you recover it. Denials are corrected and resubmitted, or appealed. Underpayments are recovered through variance disputes, payer escalation, and contract enforcement.
- Typical recovery win rate. Denials run about 50-70% depending on root cause. Underpayments hit 70-85% when appeals cite exact contract language.
Hospitals that focus only on denials and never on underpayments routinely leave 1-3% of net revenue uncollected. A complete revenue integrity program addresses both.
The six most common causes of payer underpayments
Most healthcare underpayments trace back to a handful of recurring root causes. Identifying which ones drive the most dollar loss at your organization is the first step toward systematic recovery.
1. Contract misinterpretation. Payer contracts run hundreds of pages with layered fee schedules, exceptions, and carve-outs. Payer systems are configured by humans and routinely misread complex language - especially around case rates, stop-loss, and outlier provisions.
2. Outdated payer fee schedules. When CMS or commercial rates change, payer adjudication engines don't always update immediately. The result is silent underpayment against the contracted (current) rate.
3. Improper bundling or unbundling. Payers bundle services that should pay separately - or apply edits like NCCI that suppress legitimate line items. Each instance is a small dollar variance that compounds across thousands of claims.
4. Modifier and code-edit errors. Missing modifier 25 or 59, incorrect units, or wrong place-of-service codes trigger automatic downcoding or partial denial. Some of these are clinic-correctable; others are payer errors that must be appealed.
5. "Lesser of" clauses on the chargemaster. Many contracts pay the lesser of the contracted rate or the billed charge. If your chargemaster sets a charge below the contracted rate, the payer pays the lower amount - and that gap is permanent revenue loss unless the chargemaster is restructured.
6. Silent partial payments. Sometimes payers simply remit less than the contracted amount with no remark code, no denial signal, and no explanation. Only a variance engine that knows the contract terms can catch this category.
The 5-step underpayment collections process
A mature underpayment collections program follows a repeatable workflow. Each step is necessary; skipping any one of them leaves dollars on the table or recreates the same leakage next quarter.
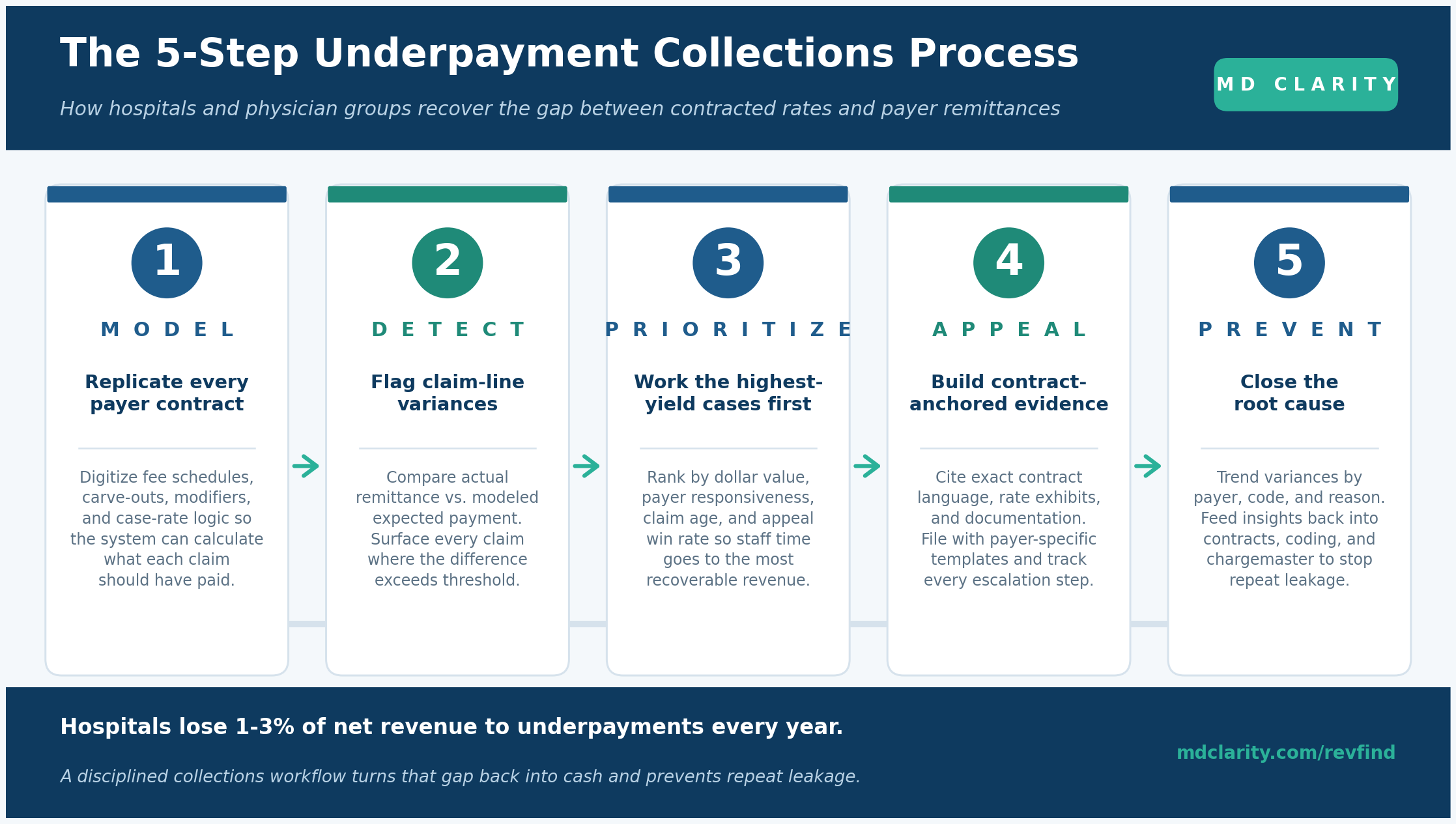
Step 1. Model expected reimbursement from the contract
You can only spot a variance if you know what the claim should have paid. That means digitizing every executed payer contract - fee schedules, carve-outs, modifiers, locality adjustments, case rates, stop-loss thresholds, lesser-of clauses - and keeping Medicare and other reference rates current. This is the foundational layer, and the precision of everything downstream depends on it.
Step 2. Detect claim-line variances
Compare every line of every remittance against the modeled expected payment. Flag claims where the difference exceeds a defined dollar or percentage threshold. The detection has to happen at the line level, not the claim level - bundling errors and modifier issues are invisible at higher aggregation.
Step 3. Prioritize by recoverable value
Not every variance is worth pursuing. Rank work items by dollar amount, payer responsiveness, claim age (against timely-filing limits), and historical appeal win rate. You can decide to work single-line variances above $25 individually and batch-appeal systemic issues that produce many small variances on the same code.
Step 4. Appeal with contract-anchored evidence
Successful underpayment appeals are specific. They reference contract language, rate exhibits, and timelines rather than generic complaints. Build payer-specific templates that include the member and claim identifiers, a clear statement of variance (expected vs. actual allowed amount), the exact contract section that supports your position, and the timely-appeal deadline. Track every escalation step, including direct payer negotiations and coordination with legal counsel when necessary.
Step 5. Collect, then prevent recurrence
Once dollars come back, the work isn't done. Trend variances by payer, procedure code, and denial reason. Feed those insights into contract renegotiation, coding education, and chargemaster adjustments. A single payer with a recurring systemic underpayment pattern is a far more valuable finding than a one-off $30,000 appeal - it's the kind of insight that turns underpayment collections into a strategic revenue function.
Anatomy of a winning underpayment appeal
The single biggest predictor of recovery success is the quality of the appeal packet. Generic letters demanding "review" of an underpaid claim usually get a generic reply. Contract-anchored appeals that quote the exact rate exhibit and cite the precise variance get paid. The packet should include, at minimum:
- Claim identifiers: member name, claim number, date of service, billing provider NPI.
- Variance statement: expected allowed amount per the contract, actual allowed amount per the remittance, dollar and percentage gap.
- Contract citation: the specific section, fee schedule line, or rate exhibit that supports the expected amount.
- Supporting documentation: the EOB or ERA, the relevant medical records or coding rationale, the executed contract page where the rate is defined.
- Filing route and deadline: the payer-specific dispute or variance channel, and the timely-filing window.
This is why one multispecialty clinic recovered $250,000 over 18 months simply by cross-referencing every variance against the contract's fee schedule before filing. The legal leverage isn't theoretical: payers are in violation of an executed contract, and disciplined providers can hold them to it.
The KPIs that actually matter
If you can't measure underpayment collections, you can't improve it. The metrics that distinguish mature programs from ad-hoc ones:
- Total variance identified ($ and % of NPR): the dollar value of underpayments your system surfaces each month. Track it gross, not net of disputes.
- Variance recovery rate: dollars recovered divided by dollars identified. Mature programs target 65-80%.
- Appeal win rate: appeals upheld in your favor. Above 70% is achievable when appeals are contract-anchored.
- Days from identification to recovery: tighter is better; under 60-90 days is a reasonable target.
- Recovered dollars per FTE: a productivity measure that informs staffing decisions.
- Repeat-leakage rate by payer and code: the prevention metric. A rising number here means the root cause isn't getting fixed.
Build it in-house, buy software, or partner with experts?
There is no single right answer; the decision depends on your team's size, payer mix, contract complexity, and current backlog. A useful frame:
- Software-only (build the team, buy the engine): the right path for providers with experienced contract management staff and managed-care leadership. You retain control of the appeal workflow and capture all the institutional knowledge in-house.
- Full-service partner: the right path for providers with a meaningful backlog, limited specialist headcount, or complex commercial payer mixes. You get faster ROI because specialists handle detection, appeals, and escalation end-to-end.
- Hybrid: increasingly common - use software for the steady-state work and bring in a service partner to clear backlogs or tackle high-complexity payers.
How MD Clarity supports both paths
MD Clarity's platform is built around the workflow above and gives you two ways to put it to work.
RevFind is the revenue optimization software. Use it to replicate payer adjudication with charge-level precision, surface underpayments and denials into prioritized worklists, and digitize your full contract portfolio for ongoing variance detection and modeling.
Underpayment Recovery Services is the RevFind-enabled service. Specialists analyze every flagged variance, assemble contract-anchored appeals, and pursue each case through escalation, so you get recovered cash without adding headcount.
FAQs
What is the difference between underpayment collections and denial management?
Denial management addresses claims that were explicitly rejected (in full or part) by the payer with a denial code on the remittance. Underpayment collections addresses claims that were paid, but at less than the contracted rate, with no denial code attached. Different detection method, different recovery workflow, different team owner.
How much of net patient revenue do hospitals typically lose to underpayments?
Most published benchmarks place commercial-payer underpayments at 1% to 3% of net patient revenue annually. Some estimates run to 5%, particularly for organizations with high payer complexity or weak contract enforcement. Medicare and Medicaid underpayments are a separate (and much larger) category driven by below-cost statutory rates.
What is the most common cause of payer underpayments?
It varies by organization, but contract misinterpretation, outdated payer fee schedules, and improper bundling are the three most frequent dollar drivers. Lesser-of clauses against the chargemaster are the most often-overlooked structural cause and can produce systematic leakage that no appeal will recover - only a chargemaster restructure will.
How do you build a successful underpayment appeal?
Cite the exact contract clause, fee schedule, or rate exhibit that supports the expected payment, include the variance calculation (expected vs. actual allowed amount), and attach the supporting documentation (EOB, medical records, contract page). Generic complaints get generic responses; contract-anchored appeals get paid.
What software do hospitals use for underpayment collections?
Hospitals use contract management and payment variance platforms that can replicate payer adjudication at the claim-line level, including modifiers, locality adjustments, carve-outs, and case rates. MD Clarity's RevFind is one example; others on the market include legacy contract management systems and newer revenue intelligence platforms. The key requirement is that the engine must mirror payer logic with charge-level precision.
Is it worth outsourcing underpayment collections?
For providers with backlogs, limited contract specialists, or complex commercial payer mixes, yes - a technology-enabled service partner typically delivers positive ROI within the first recovery cycle by addressing high-value variances first. Providers with mature managed-care teams and existing contract modeling capability are often better served by purpose-built software they can run themselves.
Get paid in full by bringing clarity to your revenue cycle
Related Posts


Subscribe to the

Healthcare Clarified newsletter
Get the latest insights on RCM and healthcare policy in your inbox
