.avif)
.svg)
.svg)
Hospital patient estimates have moved from a nice-to-have customer service touch to a regulated, revenue-critical workflow. With the No Surprises Act in force, the CY 2026 hospital price transparency rule now in effect, and Executive Order 14221 sharpening enforcement, every hospital that schedules services needs a clear process for telling patients what their care will cost - before they arrive.
This guide explains exactly what hospital patient estimates are, what regulations require, who qualifies, what must be included, and how leading provider organizations are automating the process to stay compliant and protect margins.
What Are Hospital Patient Estimates?
A hospital patient estimate is a written projection of the expected charges for the items and services a patient is scheduled to receive. For uninsured and self-pay patients, this estimate takes a regulated form called a Good Faith Estimate (GFE), required under the No Surprises Act. For insured patients, hospitals typically generate out-of-pocket cost estimates using payer eligibility data, contracted rates, and the patient's deductible and coinsurance status.
In short: hospital patient estimates translate complex chargemaster, contract, and benefits data into a single, plain-language number a patient can plan around.
Why Hospital Patient Estimates Matter More Than Ever
Patient financial responsibility is now roughly 30% of provider revenue, driven by the spread of high-deductible plans. The average single-coverage deductible reached $1,886 in 2025, and out-of-pocket hospital spending is projected to rise about 3.2% per year through 2033.
When patients cannot see what they will owe, they react in ways that hurt both their health and the hospital's bottom line:
- Roughly 73% of providers report patients delay or skip care when they cannot get an upfront cost estimate.
- Close to half of patients say they will not seek care without understanding what it will cost.
- 46% of patients stop treatment after receiving an estimate they perceive as too high.
- Provider bad debt write-offs hit $17.4 billion in 2023, with 53% of those write-offs coming from insured patients.

Accurate estimates flip these numbers. One health system using automated patient estimates boosted pre-service collections by 47% while reducing surprise bills.
What Regulations Require Hospital Patient Estimates?
Three federal frameworks govern hospital patient estimates today.
1. The No Surprises Act (effective January 1, 2022)
The No Surprises Act requires hospitals, physicians, and most other licensed facilities to provide Good Faith Estimates to uninsured and self-pay individuals for scheduled care. The rule is codified at 45 CFR 149.610 and is enforced by the Centers for Medicare and Medicaid Services (CMS), with state-level enforcement in most jurisdictions.
2. The Hospital Price Transparency Rule (effective January 1, 2021)
The Hospital Price Transparency Rule requires hospitals to publish a machine-readable file of standard charges and either a consumer-friendly shoppable services display or a price estimator tool. The CY 2026 OPPS Final Rule tightened these requirements substantially, replacing estimated allowed amounts with actual median, 10th, and 90th percentile dollar amounts drawn from real claims data. Enforcement of the revised requirements began April 1, 2026.
3. Executive Order 14221 (February 2025)
Executive Order 14221, titled "Making America Healthy Again by Empowering Patients with Clear, Accurate, and Actionable Healthcare Pricing Information," directed HHS to require the disclosure of actual prices rather than estimates in machine-readable files, standardize pricing data for cross-hospital comparison, and bolster enforcement. CMS fined 10 hospitals in 2025 alone, with civil monetary penalties ranging from $32,301 to $309,738 per hospital.
The insured-patient Advanced Explanation of Benefits (AEOB) requirement remains delayed pending future rulemaking, but hospitals are wise to build estimate workflows that can support it when enforcement begins.
Who Is Entitled to a Hospital Patient Estimate?
Under current No Surprises Act enforcement, three groups must receive a Good Faith Estimate:
- Uninsured patients scheduling any service at least three business days in advance
- Self-pay patients - including insured individuals who choose not to bill their insurance
- Any patient who requests an estimate before scheduling
Federal program beneficiaries (Medicare, Medicaid, TRICARE, Veterans Affairs, Indian Health Services) are excluded because these programs have other protections against high medical bills.
For insured patients, hospitals are not yet federally required to deliver a written estimate, but state laws, contractual obligations, and patient expectations increasingly demand one.
When Must Hospitals Deliver Patient Estimates?
The No Surprises Act sets specific deadlines tied to how far in advance a service is scheduled.

The three scenarios:
- Scheduled 10 or more business days in advance: estimate due within 3 business days of scheduling
- Scheduled 3 to 9 business days in advance: estimate due within 1 business day of scheduling
- Patient-requested estimate: due within 3 business days of the request
If anything material changes after the estimate is issued - expected charges, providers, scope, or dates - the hospital must issue an updated estimate at least one business day before service.
Services scheduled fewer than three business days in advance are not subject to the GFE requirement, which is why most walk-in and emergency encounters are exempt.
What Must Be Included in a Hospital Patient Estimate?
A compliant Good Faith Estimate is not just a dollar figure. CMS specifies eight categories of required content.
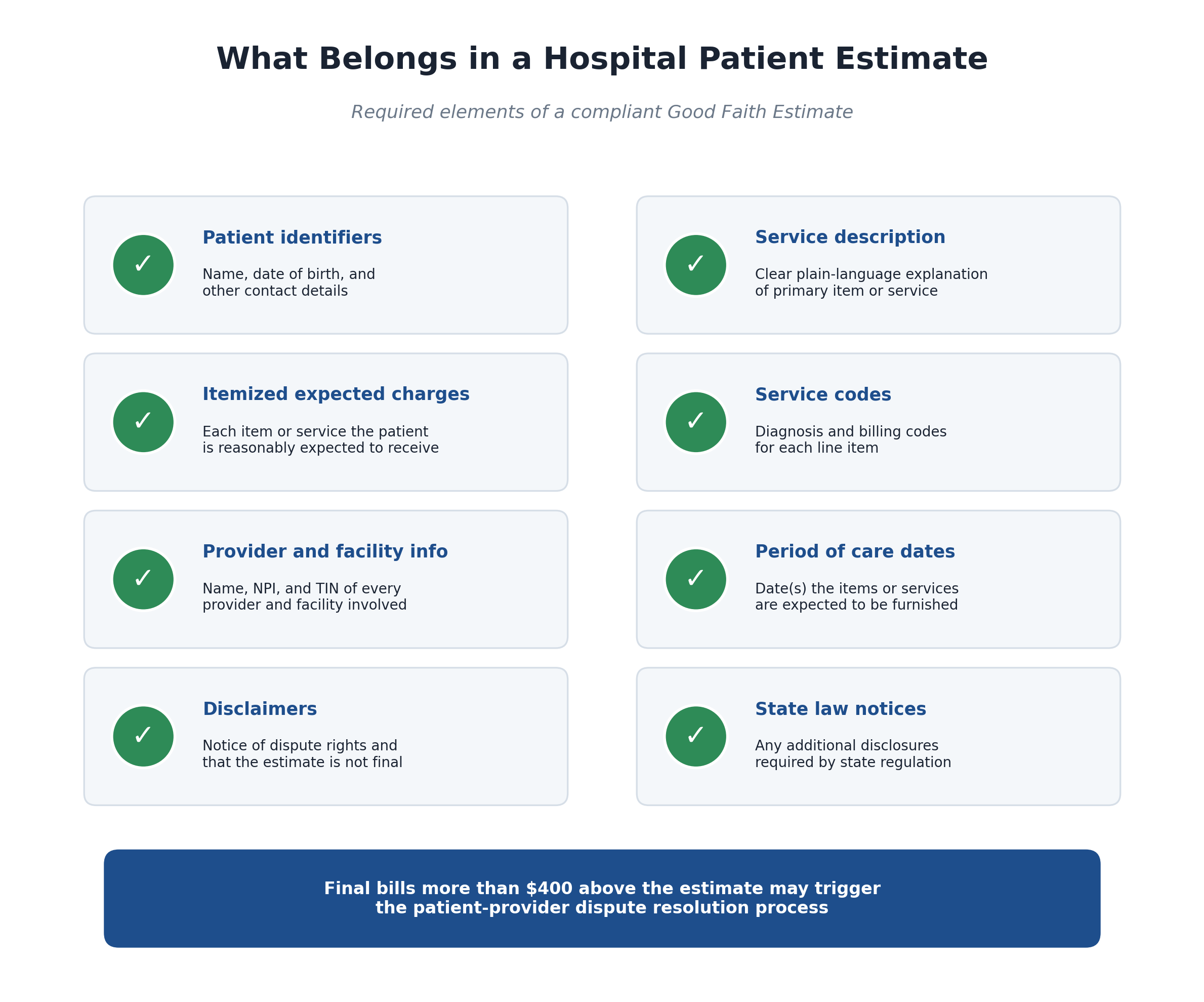
The required elements are:
- Patient identifiers: name, date of birth, and contact information
- Plain-language service description: a clear explanation of the primary item or service
- Itemized expected charges: every item or service the patient is reasonably expected to receive
- Service codes: diagnosis and billing codes for each line item
- Provider and facility information: name, National Provider Identifier (NPI), and Taxpayer Identification Number (TIN) for every provider and facility involved
- Period of care dates: the day or days on which items and services will be furnished
- Disclaimers: a notice of the patient's right to dispute charges and a statement that the estimate is not a binding contract
- State law notices: any additional disclosures required by the state in which the service is rendered
The estimate must also reflect any expected discounts the hospital plans to apply, such as financial assistance program adjustments under a tax-exempt hospital's Financial Assistance Policy.
How Accurate Do Hospital Patient Estimates Need to Be?
The No Surprises Act creates a dispute path for patients whose final bills exceed their estimate by more than $400 per provider. Under the patient-provider dispute resolution (PPDR) process, the patient can submit the bill to HHS for review by a Selected Dispute Resolution (SDR) entity.
The standard is "reasonably expected" charges based on information available at the time of scheduling. Hospitals are not penalized for unforeseeable changes in scope - but they are responsible for errors and omissions in what was knowable when the estimate was issued.
Independent surveys, however, suggest accuracy has been declining. According to Experian Health, 88% of providers say improving estimate accuracy is urgent, and patient-reported estimate accuracy has fallen for three consecutive years.
What Are the Penalties for Non-Compliance?
Penalties come from two distinct frameworks.
Under the No Surprises Act, HHS can require corrective action plans and impose civil monetary penalties of up to $10,000 per violation. Most enforcement is delegated to states.
Under the Hospital Price Transparency Rule, CMS calculates penalties daily, scaled to hospital size. As of 2025, fines ranged from $32,301 to $309,738 per enforcement cycle, and CMS began publicly naming non-compliant organizations. The CY 2026 rule offers a 35% civil monetary penalty reduction when hospitals waive their right to an administrative hearing - but only for non-core violations.
The reputational risk often outweighs the dollar penalty. Public dashboards comparing hospital compliance are now part of the consumer healthcare landscape.
Common Challenges Hospitals Face with Patient Estimates
Even well-intentioned hospitals routinely struggle in five areas.
1. Time per estimate. CMS itself estimates that compiling one patient payment estimate can take up to 1.3 hours when done manually. At any meaningful patient volume, this is unsustainable.
2. Co-provider and co-facility coordination. Surgeries and complex services involve multiple billers - the surgeon, anesthesiologist, pathologist, hospital, and ambulatory facility. The "convening provider" must aggregate estimates from all of them, and there is no national standard system for exchanging this information.
3. Eligibility and benefits data freshness. Patient cost depends on plan design, deductible status, coinsurance, and authorization. Pulling stale data leads to inaccurate estimates and dispute risk.
4. Multi-state operations. Many hospitals operate across states with different price transparency laws. A single estimate template rarely satisfies every jurisdiction.
5. Staffing. Manually generating compliant estimates at scale typically requires four to eight additional FTEs for a mid-sized organization - an added cost of $172,000 to $344,000 per year at $43,000 in fully loaded compensation per medical billing specialist.
Best Practices for Accurate Hospital Patient Estimates
Hospitals that consistently produce accurate, timely estimates share a handful of operational practices.
Verify eligibility in real time. Pulling live 270/271 data at scheduling and again shortly before service catches deductible movement, plan changes, and authorization issues before they become estimate errors.
Use contracted rates, not chargemaster. Estimates built on negotiated rates - layered with each patient's specific deductible and coinsurance - are dramatically more accurate than chargemaster-based projections.
Trigger estimates automatically at scheduling. The fastest path to compliance is removing the human "send" step entirely so that every scheduled patient receives an estimate within the regulatory window.
Deliver through multiple channels. Patients prefer different channels. Email, secure text, and mailed letter together capture nearly every recipient.
Embed a payment link. When the estimate doubles as a payment portal, patients can put down a deposit or pay in full from home, which reduces no-shows and bad debt.
Track changes and reissue. Build alerts that reissue an estimate the moment scope, providers, or expected charges change.
Document everything. Retain estimates, delivery confirmations, and any updates for the full audit trail. CMS expects this.
How Automation Transforms Hospital Patient Estimates
Manual estimate workflows simply do not scale to current regulatory demands. The hospitals navigating this best have shifted to platforms that automatically pull eligibility, apply contracted rates, generate compliant Good Faith Estimates, and deliver them through the patient's preferred channel - all without staff clicks.
Automation delivers four compounding benefits:
- Compliance: every scheduled patient receives a timely, complete estimate that meets No Surprises Act and state requirements
- Speed: hour-long manual estimates collapse to seconds
- Accuracy: real-time eligibility and contracted rates reduce dispute risk
- Cash acceleration: embedded payment links convert estimates into deposits, shrinking accounts receivable and bad debt
How Clarity Flow Streamlines Hospital Patient Estimates and No Surprises Act Compliance
MD Clarity's Clarity Flow is patient estimate software purpose-built for this moment. It turns insurance benefits, contracted rates, and service details into accurate, compliant patient cost estimates - and delivers them automatically.
What Clarity Flow does for hospitals and provider organizations:
- Automates Good Faith Estimates end-to-end, generating and sending GFEs by text, email, or letter on the exact timeline the No Surprises Act requires
- Verifies eligibility and benefits in real time so estimates reflect each patient's actual deductible and coinsurance status
- Applies contracted rates rather than chargemaster prices for substantially higher accuracy
- Embeds secure payment links in every estimate, so patients can place a deposit, pay in full, or enroll in a payment plan directly from the document
- Integrates with existing systems through APIs and HL7/FHIR connections to platforms such as Epic, athenahealth, ModMed, eClinicalWorks, and NextGen
- Handles multi-state complexity with configurable templates for the specific disclosures each state requires
- Eliminates the manual spreadsheet work behind No Surprises Act compliance
One women's health group used Clarity Flow to send 445 compliant Good Faith Estimates per day without adding staff, avoiding $172,000 to $344,000 in annual hiring costs. Most clients see 99% of estimates deploy automatically with no staff intervention.
For hospitals facing tightened CMS enforcement, rising patient responsibility, and the daily reality that every aging dollar gets harder to collect, Clarity Flow turns hospital patient estimates from a compliance burden into a revenue advantage.
Book a demo of Clarity Flow to see how automated patient estimates can protect compliance, cash flow, and the patient experience at the same time.
Frequently Asked Questions
Are hospital patient estimates legally required?
Yes, for uninsured and self-pay patients. The No Surprises Act requires hospitals to provide a Good Faith Estimate to any uninsured or self-pay individual who schedules a service at least three business days in advance, or who requests an estimate. Hospital price transparency rules separately require public disclosure of negotiated rates and either a shoppable services display or a price estimator tool.
Do hospital patient estimates apply to insured patients?
Federal Good Faith Estimate requirements for insured patients - and the related Advanced Explanation of Benefits requirement - remain delayed pending future rulemaking. Many hospitals still produce out-of-pocket estimates for insured patients as a best practice, and state laws may require them.
What happens if the final bill is higher than the estimate?
If the final bill exceeds the estimate by more than $400 per provider, an uninsured or self-pay patient can initiate the patient-provider dispute resolution process through HHS. A Selected Dispute Resolution entity then reviews whether the additional charges were reasonable and medically necessary based on what was knowable at scheduling.
Are emergency services subject to GFE requirements?
No. Good Faith Estimates are required only for scheduled services. Walk-in, urgent care, and emergency services are not subject to GFE timing requirements because they cannot be scheduled three business days in advance.
How accurate must hospital patient estimates be?
There is no specific accuracy percentage in the regulation, but estimates must reflect charges the hospital "reasonably expects" based on the information available at scheduling. Bills more than $400 above the estimate per provider can trigger patient-initiated dispute resolution, so most hospitals target accuracy well inside that threshold.
Can hospital patient estimates include co-provider charges?
Yes - and ultimately they must. The "convening provider" or "convening facility" is responsible for aggregating expected charges from co-providers and co-facilities involved in a period of care. CMS has exercised enforcement discretion on this element, but provider organizations should be building toward fully aggregated estimates today.
How long do hospitals have to retain patient estimates?
Hospitals should retain Good Faith Estimates, delivery confirmations, and any updates as part of their compliance records. While CMS has not specified a single retention period, six years aligns with general HIPAA documentation guidance and is widely recommended.
FAQs
Get paid in full by bringing clarity to your revenue cycle
Related Posts
.avif)

Subscribe to the

Healthcare Clarified newsletter
Get the latest insights on RCM and healthcare policy in your inbox
