.avif)
.svg)
.svg)
What a modern estimator actually computes, why industry accuracy is dropping, and how to evaluate the software that will become a 2026 regulatory must-have.
A patient payment estimator is software that produces a pre-service estimate of what a patient will owe out-of-pocket for a scheduled visit or procedure. It pulls registration data from the practice management system, runs a real-time benefits check, applies contracted payer rates and fee schedules, factors in modifiers and lesser-of clauses, and returns a clear dollar breakdown delivered to the patient digitally - all before service is rendered. When the estimate is accurate, patients pay sooner and forgo care less often. When it is not, both sides lose: industry estimate accuracy dropped from 78% in 2022 to 71% in 2025, and patient confidence has eroded with it.
Key takeaways
- Accuracy is declining. Estimate accuracy fell 7 percentage points in three years, from 78% in 2022 to 71% in 2025, even as more patients receive estimates.
- An eligibility check is not an estimate. A benefits lookup tells you the patient's deductible status; it does not tell you what the payer will pay. Without contracted rates, the number on the patient's statement is a guess.
- Six data inputs feed every accurate estimate. Registration data, real-time benefits, contracted rates, reference fee schedules, chargemaster pricing, and prior balance.
- The financial impact is large. 78% of providers fail to collect a $1,000 balance within 30 days. Pre-service estimates with a pay-now link shift that math significantly.
- The 2026 transparency rules raised the stakes. The Hospital Price Transparency Rule update took effect January 1, 2026, with enforcement starting April 1. Audit-ready estimator output is no longer optional.
What is a patient payment estimator?
A patient payment estimator is the software layer that sits between the patient access workflow and the financial conversation. Its job is to answer one question accurately and on time: what will the patient owe out-of-pocket for this scheduled service?
Modern estimators differ sharply from the price calculators of five years ago. Those earlier tools typically returned a "list price" or a charge-based estimate that bore little resemblance to what the patient actually owed after insurance. A current-generation estimator combines:
- Registration data from the practice management system (procedure CPT codes, modifiers, payer, provider, place of service).
- Real-time benefits from the payer (current deductible balance, remaining out-of-pocket maximum, coinsurance, copay, accumulator status).
- Contracted payer rates from a digitized contract repository (fee schedules, case rates, anesthesia formulas, carve-outs, lesser-of clauses).
- Reference fee schedules (current Medicare RBRVS with locality adjustments and sequestration; commercial reference rates).
- Chargemaster pricing (especially for contracts with lesser-of language).
- Prior balance and accumulator history (outstanding balances, payment plan obligations, prior-service deductible application).
The output is a patient-friendly digital statement showing exactly how the total breaks down into deductible, copay, and coinsurance components, with a pay-now link and the required Good Faith Estimate disclaimers built in.
Why estimate accuracy is getting worse, not better
Counterintuitively, estimates have become more common but less accurate over the last three years. Experian Health's 2025 State of Patient Access survey found that 41% of patients received an estimate in 2025 (up from 29% in 2022), but accuracy dropped from 78% to 71% over the same period. Providers know it: 88% told the same survey that improving estimate accuracy is an urgent priority.
The structural reason is data complexity. The benefits side is moving (higher deductibles, more cost-sharing variations, more plan designs), the contract side is moving (more case-rate arrangements, more modifier-sensitive logic), and the regulatory side keeps adding requirements. Spreadsheet-based estimates and eligibility-only tools cannot keep up.

Each of these six layers represents a place where an estimate can quietly fail. Drop any one of them and the result is the kind of estimate the patient calls billing about three weeks after the visit.
The estimator capability spectrum
Not every tool calling itself a "patient payment estimator" actually computes the same things. The market spans four distinct levels of capability, and the difference between them shows up directly in accuracy.
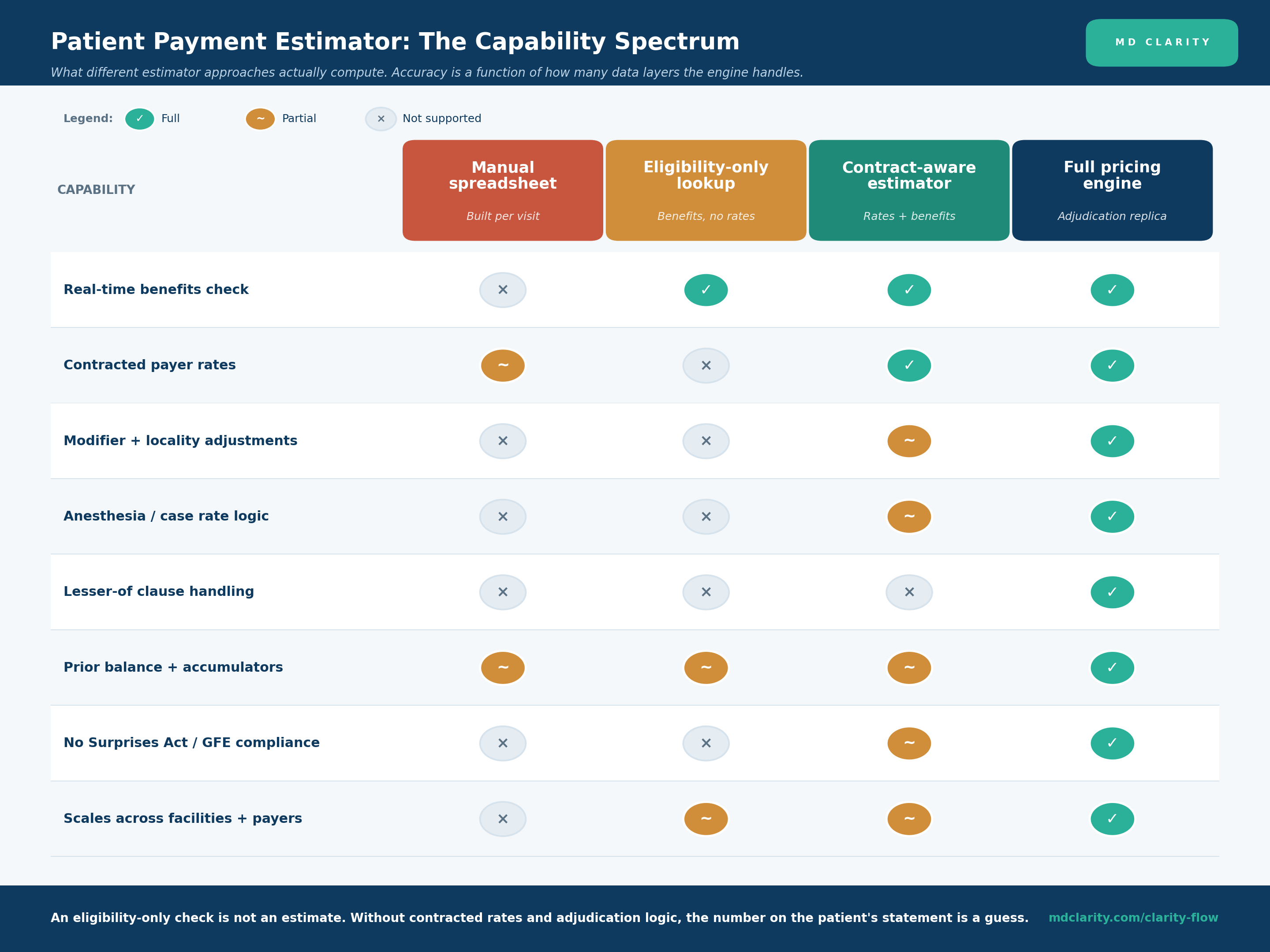
- Manual spreadsheet. Built by staff per visit. Uses static rate tables that go stale within a quarter. Cannot handle real-time benefits or modifier logic at scale. Useful only for the smallest single-payer practices.
- Eligibility-only lookup. Returns benefits data (deductible, copay, coinsurance) but does not apply contracted rates. Produces a "best guess" that ignores what the payer will actually allow. The improvement over manual is speed, not accuracy.
- Contract-aware estimator. Combines benefits with a contract repository. Handles basic fee schedules well. Modifier and anesthesia logic varies by vendor; lesser-of handling is typically weak.
- Full pricing engine. Replicates payer adjudication at the charge line. Applies modifiers, locality adjustments, case rates, and lesser-of policies. Tracks accumulators across services. Delivers audit-ready estimates that hold up under No Surprises Act scrutiny.
The gap between the second and fourth columns is where most of the industry accuracy decline lives. An eligibility-only check is not an estimate. Without the contracted rates and adjudication logic, the dollar figure on the patient's statement has no structural relationship to what they will eventually owe.
The end-to-end estimate workflow
A patient payment estimator is more than the moment of calculation. The workflow it lives in covers six steps from scheduling to post-service reconciliation.
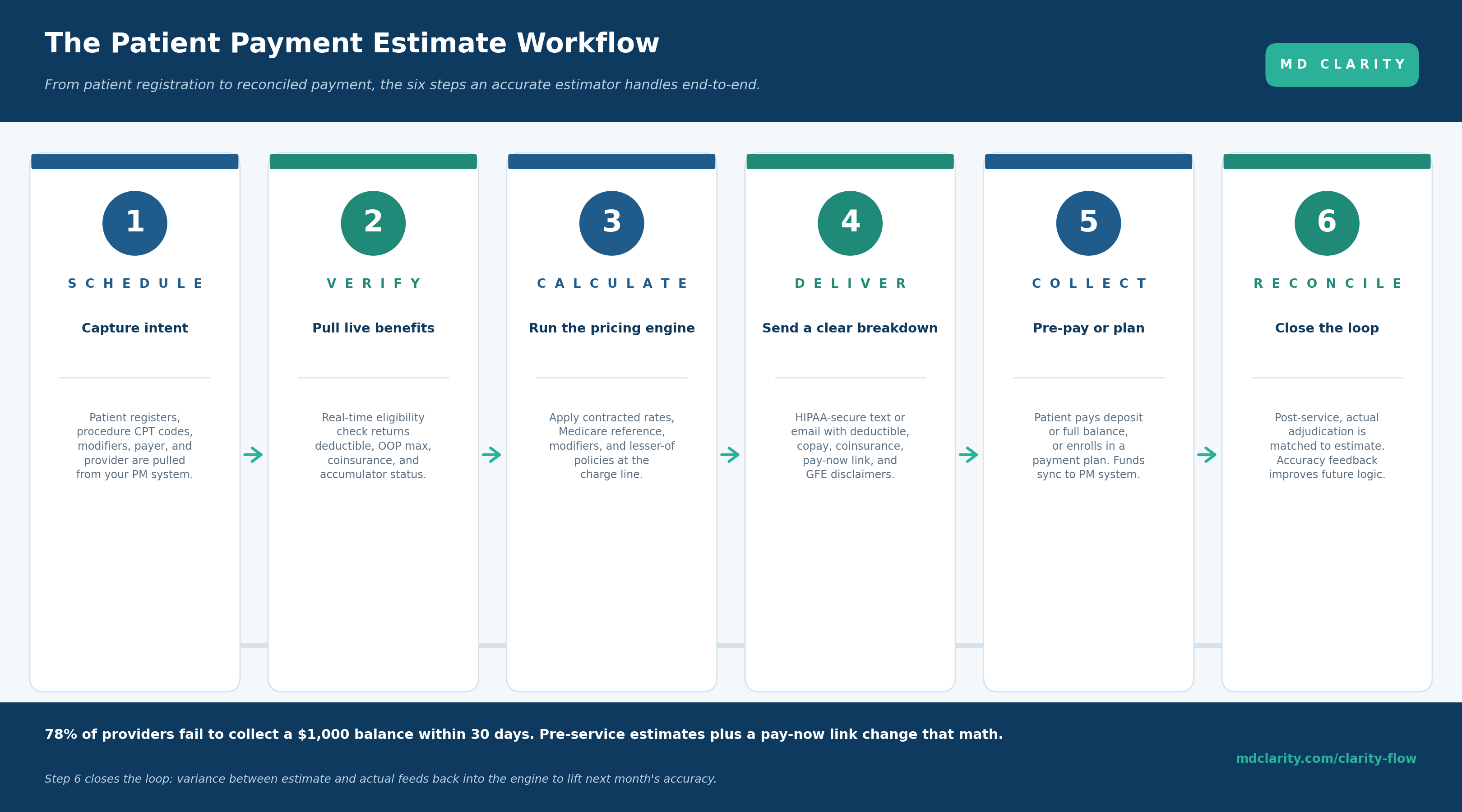
1. Schedule. Patient registers. CPT codes, modifiers, payer, provider, and place of service flow into the estimator from the PM system in real time.
2. Verify. A real-time eligibility check returns the current deductible balance, remaining out-of-pocket maximum, coinsurance and copay structure, and any plan-level accumulator data.
3. Calculate. The pricing engine applies the contracted rates, factors in modifiers and locality adjustments, runs the lesser-of comparison against the chargemaster, and computes the expected allowed amount and patient responsibility at the charge-line level.
4. Deliver. The estimate goes out via HIPAA-secure text or email with a clear breakdown (deductible, copay, coinsurance), a pay-now link, branded letter formatting, and the required Good Faith Estimate disclaimers.
5. Collect. Patient pays a deposit or the full balance through the portal, or enrolls in a payment plan. Payments sync back to the PM system without staff intervention.
6. Reconcile. After service, actual adjudication is matched against the estimate. Variance feedback flows back into the pricing engine to lift accuracy on similar future estimates.
Step 6 is the one most teams skip and the one that distinguishes a mature program from a one-time implementation. Estimate accuracy is a learning loop, not a static metric.
The No Surprises Act and GFE compliance dimension
Patient payment estimators are no longer just a collections optimization. Since January 1, 2022, the No Surprises Act has required providers to deliver Good Faith Estimates to uninsured and self-pay patients within defined timelines. The Hospital Price Transparency Rule update took effect January 1, 2026, with enforcement beginning April 1, 2026.
What that means operationally:
- Required timelines. GFEs must be delivered within specific windows depending on when service is scheduled. A compliant estimator handles the timing automatically rather than requiring staff calendars.
- Required disclaimers. Specific regulatory language must appear on each estimate. Hardcoded templates eliminate the staff judgment that creates noncompliance risk.
- Machine-readable output. Certain estimate categories must be formatted for machine consumption. The estimator should produce these files automatically.
- Audit trail. Every estimate generated, delivered, and acted on needs a defensible log. Manual tracking is the most common point of failure under CMS audit.
The penalty risk has gone from theoretical to active. An estimator with built-in GFE compliance is no longer a nice-to-have for any provider organization that bills self-pay patients.
What to look for when evaluating a patient payment estimator
Beyond the six capabilities above, a few requirements separate enterprise-grade estimator software from feature-list demos that struggle in production:
- Charge-line precision, not aggregate approximation. Anything coarser misses the modifier and lesser-of logic where most accuracy errors hide.
- Native Medicare and commercial reference rule maintenance. The vendor should keep CMS fee schedules, locality adjustments, sequestration, and similar reference data current. That cannot be a customer-managed configuration burden.
- Self-service AND full-service contract loading. Both paths are useful: self-service for quick edits as terms change, full-service onboarding for a large portfolio.
- Touchless delivery. Estimates should flow to patients via secure text or email based on rule logic, with staff only intervening when registration data is incomplete.
- Branded patient experience. The estimate the patient sees is part of the brand. Customizable letter templates with the provider's logo and tone matter for both satisfaction and pay-now conversion.
- Multi-facility, multi-source ingestion. Most provider organizations have more than one PM system. The estimator needs to handle that natively, not via spreadsheet bridges.
- A complete audit trail. Every estimate, every disclaimer, every delivery confirmation, retained per CMS audit standards.
KPIs to measure estimator success
Estimator software without measurement is just another patient-access tool. The metrics that distinguish a working program:
- Estimate accuracy. Percentage of estimates within $10 or 5% of the actual billed amount. A published JAMA Network Open study of a real-world fee estimator hit 83.9% on this definition. Aim above 80%.
- Pre-service collection rate. Dollar value collected before service divided by total expected patient responsibility on those visits.
- Point-of-service collection rate. Patient dollars collected before walking out the door.
- Estimate-to-pay conversion. Percentage of delivered estimates that result in any payment within seven days.
- Estimate delivery rate. Percentage of eligible visits that receive an estimate. Even mature programs leave 20-40% of visits uncovered without specific operational attention.
- Staff time per estimate. With automation, this should approach zero for the standard case. The MD Clarity product sheet for Clarity Flow cites a 95%+ reduction in manual work as the benchmark.
- 30-day collection on balances over $1,000. The industry baseline is brutal: 78% of providers fail to collect a $1,000+ balance within 30 days, per MGMA and industry studies compiled in the Clarity Flow research. Pre-service estimates with embedded pay-now links are the primary lever to move this number.
Build, buy, or partner
Building a pricing engine that replicates payer adjudication is a multi-year engineering project with permanent maintenance overhead as fee schedules, modifiers, and policies change. Almost no provider organization gets a positive return on that investment versus buying.
The realistic choice is between purpose-built estimator software you operate, and a service partner who operates it for you:
- Software you operate. The right path for provider organizations with experienced patient access and managed-care teams who want operational control.
- Service partner. The right path for organizations with limited specialist headcount, an aggressive transparency-compliance timeline, or complex multi-facility data ingestion needs.
- Hybrid. Software for steady-state, with a partner for onboarding, contract loading, and accuracy tuning.
How MD Clarity supports both paths
MD Clarity's pricing engine - the same one that powers contract variance detection on the back end - sits at the center of an estimator product built for both paths.
Clarity Flow is the upfront collections and price transparency software. Use it to digitize payer contracts and fee schedules, run real-time benefits checks, calculate charge-line accurate estimates, deliver them via HIPAA-secure text or email with pay-now links, and maintain a complete No Surprises Act audit trail. Touchless workflows route only exception cases to staff, cutting estimate prep time by 95%+.
For end-to-end revenue optimization, Clarity Flow pairs with RevFind, MD Clarity's revenue optimization platform that uses the same pricing engine to detect underpayments, denials, and contract mismatches after the fact. Together they cover both ends of the revenue cycle: an accurate estimate before service and a contract-anchored variance recovery after.
FAQs
What is a patient payment estimator?
A patient payment estimator is software that produces a pre-service estimate of what a patient will owe out-of-pocket. It combines six data inputs - registration data, real-time benefits, contracted payer rates, reference fee schedules, chargemaster pricing, and prior balance - to calculate the estimated patient responsibility and deliver it digitally before service is rendered.
How accurate are patient payment estimates today?
Industry accuracy fell from 78% in 2022 to 71% in 2025, according to Experian Health's State of Patient Access survey. A well-designed estimator in a published JAMA Network Open study achieved 83.9% accuracy, defined as within $10 or 5% of the actual billed amount. The gap between current industry performance and best-in-class is roughly 13 percentage points.
What is the difference between an eligibility check and a patient payment estimate?
An eligibility check returns insurance status and benefits details: deductible balance, copay, coinsurance, out-of-pocket maximum. A patient payment estimate uses those benefits plus contracted payer rates, modifiers, locality adjustments, lesser-of clauses, and chargemaster data to calculate the actual dollar amount the patient will owe. Eligibility-only tools cannot produce an accurate estimate because they do not know what the payer will pay.
Do patient payment estimators help with No Surprises Act compliance?
Yes. The No Surprises Act requires providers to deliver Good Faith Estimates to uninsured and self-pay patients within defined timelines, with specific disclaimers and a retained audit trail. A compliant estimator handles the timelines, formats estimates as machine-readable files where required, and maintains the audit log automatically rather than requiring staff to track each estimate manually.
What KPIs should we use to measure a patient payment estimator?
Track estimate accuracy (percentage within 5% or $10 of billed amount), pre-service collection rate, point-of-service collection rate, percentage of patients who receive an estimate, estimate-to-collection conversion rate, and reduction in staff time per estimate. Best-in-class programs target 80%+ accuracy and meaningfully lift pre-service collections within the first 90 days.
How does a patient payment estimator interact with practice management systems?
Through a direct integration that pulls registration data, scheduled procedure codes, modifiers, payer information, and prior balances. Output (estimates and payments) syncs back to the PM system so the financial record stays consistent. Best-in-class estimators support multiple PM systems concurrently for organizations operating across acquired practices or multi-specialty groups.
Get paid in full by bringing clarity to your revenue cycle
Related Posts


Subscribe to the

Healthcare Clarified newsletter
Get the latest insights on RCM and healthcare policy in your inbox
