.avif)
.svg)
.svg)
The 12 essential KPIs for multi-TIN MSO reporting fall into four categories: Cash & A/R (net collection rate, days in A/R, A/R over 90 days), Payer Performance (initial denial rate, underpayment rate, denial recovery rate), Operational Efficiency (clean claim rate, cost to collect, charge lag), and Patient Financial (pre-service collection rate, patient bad debt rate, estimate accuracy). Every one of these KPIs needs to roll up to platform level for the board and CFO, drill down to entity, specialty, location, payer, and provider levels for the operating teams, and refresh at the cadence each audience needs (daily for operations, weekly for revenue cycle leadership, monthly for the CFO, quarterly for the board). The reporting architecture that supports this is more complex than single-entity reporting and is one of the most under-invested capabilities at growing MSO platforms.
This guide is for MSO CFOs, VPs of revenue cycle, directors of finance, and the corporate development leaders who consume the platform-level reporting at PE board meetings. It covers what multi-TIN RCM reporting actually means, why it's harder than single-entity reporting, the four-tier audience structure, the 12 KPIs every platform needs, the benchmarks for each, and the drill-down architecture that turns platform averages into actionable signals.
What is multi-TIN RCM reporting?
Multi-TIN RCM reporting is the consolidated reporting of revenue cycle performance across every legal entity (Tax Identification Number, or TIN) in an MSO platform, with the ability to aggregate up to a platform-wide view and drill down to entity, specialty, location, payer, and provider levels. The "multi-TIN" qualifier matters because each acquired practice typically operates under its own TIN, with its own payer contracts, its own fee schedules, its own billing workflows, and often its own technology stack. Reporting that treats the platform as a single entity loses too much; reporting that stays at the entity level prevents platform-wide analysis.
The end state of multi-TIN reporting is a unified data foundation that feeds every audience in the organization: PE board members get quarterly EBITDA growth and synergy capture metrics, CFOs get monthly cash and working capital metrics, VPs of revenue cycle get weekly operational metrics, and RCM operations managers get daily cash and work-queue metrics. The same underlying data feeds all of them; what differs is the aggregation level, the cadence, and the detail.
For MSO platforms in the consolidation phase (typically Years 1 through 4 of a PE hold period), multi-TIN reporting is what makes the synergy thesis measurable. The synergy commitments made to the PE board at the start of the hold period only get tracked if the reporting infrastructure can attribute performance to specific work streams, specific entities, and specific operating decisions. Without it, the platform CFO is left explaining EBITDA variances at the board level with no underlying detail to support the explanation.
For the broader integration framework that surrounds this reporting work, see the post-acquisition revenue cycle integration playbook. For the contract consolidation work that often runs in parallel, see the multi-TIN payer contract consolidation guide.
Why multi-TIN reporting is harder than single-entity reporting
Single-entity practices have one TIN, one practice management system, one payer roster, one set of fee schedules, and one set of operating processes. Reporting at that scale is a problem most independent practices can solve with their PM system's built-in reports.
Multi-entity MSO platforms face six challenges that single-entity practices don't.
Different practice management systems. Most MSO platforms inherit a different PM system at each acquired entity (athenahealth at one, eClinicalWorks at another, NextGen at a third, Epic or Cerner at the hospital-affiliated entities). Each system has its own data model, its own report formats, and its own field definitions. A "denial" in one system isn't always the same thing as a "denial" in another.
Different fee schedules and rate methodologies. Payer contracts at each acquired entity have different rate structures (percent of Medicare, fixed dollar amounts, case rates, capitation). Calculating net collection rate consistently across the platform requires normalizing what "expected" means at each entity, which requires the contract data to be loaded at the CPT level. This is the same problem the payer contract audit work surfaces.
Different chart of accounts and revenue categorization. General ledger structures vary across acquired entities. What rolls up to "patient service revenue" in one entity may be split across multiple accounts in another. Platform-level reporting requires a consolidated chart of accounts that maps entity-level data to platform-level categories.
Specialty mix variation across entities. A multi-specialty platform with primary care, orthopedics, ophthalmology, and gastroenterology entities has dramatically different KPI expectations for each. A 45-day days-in-A/R metric is healthy for orthopedics but concerning for primary care. Platform-level reporting needs to handle the specialty mix to avoid spurious comparisons.
Credentialing and TIN complexity for providers. Providers at MSO platforms are often credentialed under multiple TINs and bill across multiple entities. Attributing claims and collections to the right provider requires cross-referencing across the platform, which adds reporting complexity.
Cash flow timing variations. Different entities have different cash posting cadences, different lockbox structures, and different banking relationships. Consolidated cash flow reporting requires mapping all of this into a unified daily, weekly, and monthly view.
The MSO platforms that invest in multi-TIN reporting infrastructure early in the hold period consistently outperform those that defer the investment. The platforms that defer typically end up rebuilding reporting from scratch around Year 3 when board pressure for sharper data forces the issue, often at significant cost.
The reporting hierarchy: from board to operations manager
The first design decision in multi-TIN reporting is recognizing that different audiences need different aggregation levels, different metrics, and different cadences. The same underlying data has to feed all four tiers without producing four different versions of the truth.

Board tier (quarterly cadence). The PE board and the platform CEO consume aggregated metrics at the platform level: platform EBITDA growth, synergy capture vs. plan, net revenue per acquired entity, EBITDA margin trend. The decisions at this tier are about strategic capital allocation, M&A timing, and exit positioning. The detail underneath the platform numbers matters less than the trends.
CFO tier (monthly cadence). The platform CFO consumes financial and operational metrics at the entity level: net collection rate by entity, days in A/R by entity, underpayment recovery rate, patient collection rate, cost to collect. The decisions are about cash flow management, working capital allocation, and payer renegotiation timing. The entity-level detail supports diagnosis of where the platform numbers come from.
VP Revenue Cycle tier (weekly cadence). The VP of revenue cycle and managed care leadership consume operational metrics at the payer and workflow level: initial denial rate by payer, aged A/R buckets by payer, credentialing status, clean claim rate, recovery queue volume. The decisions are about workflow adjustments, staff allocation, and denial escalation. The payer-level detail supports specific operational interventions.
RCM Operations Manager tier (daily cadence). The operations managers running day-to-day RCM consume granular detail at the claim, CPT, and provider level: daily cash posted vs. trailing 12-month average, denial codes by frequency, specific CPT and modifier issues, submitted claims and rejections, underpayment alerts. The decisions are about work queue prioritization and same-day cash dashboard review.
The mistake most MSO platforms make is building reporting for one tier and assuming it serves the others. CFO-level monthly reporting doesn't give operations managers the daily granularity they need. Daily operations reporting buries the CFO in detail that doesn't drive monthly decisions. Each tier needs its own report set, all feeding from the same data foundation.
The 12 essential KPIs for MSO multi-TIN reporting
The 12 KPIs that every multi-TIN MSO platform should be reporting fall into four categories. The grouping matters because the categories drive different operating decisions: cash & A/R metrics drive working capital decisions, payer performance metrics drive contract and negotiation decisions, operational efficiency metrics drive workflow and staffing decisions, and patient financial metrics drive patient access and front-end decisions.

Category 1: Cash & A/R (how fast cash flows in)
Net collection rate (benchmark: 95% or higher). Payments collected as a percentage of allowed amounts, calculated against contracted rates rather than charges. Net collection rate below 92% indicates write-offs are eating real revenue, often through unworked underpayments or aged denials. The KPI is one of the most diagnostic in the cluster because gaps trace to specific operational failures.
Days in A/R (benchmark: under 40 days). Average days from claim submission to payment, calculated across the platform. Above 50 days, working capital is locked up and cash flow becomes a problem. The KPI varies meaningfully by specialty (orthopedics tends to run higher than primary care due to procedure billing complexity), which is why platform-level reporting needs to handle specialty mix.
A/R over 90 days (benchmark: under 18% of total A/R). The share of A/R that has aged past 90 days. Above 25%, collection probability falls sharply and the practice is heading toward write-offs. This is one of the most important leading indicators of patient bad debt and one of the revenue cycle red flags that diligence teams screen for during pre-close.
Category 2: Payer Performance (how well payers honor contracts)
Initial denial rate (benchmark: under 5%). The share of claims denied on first submission, by payer. Industry research from Experian Health's annual State of Claims survey has found denials climbing to nearly 12% of submitted claims, so the under-5% benchmark requires active management. Platform-level reporting that shows denial rate by payer surfaces which payers are dragging the average and need operational attention.
Underpayment rate (benchmark: under 1% of NPR). Variance between paid amounts and contracted rates, expressed as a percentage of net patient revenue. Industry-typical underpayment exposure runs 1 to 3% of NPR for practices without continuous variance detection. Platforms that drive the rate below 1% have built systematic underpayment detection into their operating model.
Denial recovery rate (benchmark: above 70%). The share of denied claims successfully overturned on appeal. Industry research from the AMA's denial reform initiative and others suggests that 60-65% of denials are appealable, and well-run revenue cycle operations recover the majority of those. Below 50% recovery, the platform is leaving real money on the table to time and timely filing limits.
Category 3: Operational Efficiency (how well the work flows)
Clean claim rate (benchmark: above 95%). The share of claims accepted on first submission without payer rejection. Below 90%, the platform has front-end issues (eligibility, coding, charge capture) that are creating rework downstream. The KPI directly affects cost to collect because rework is expensive.
Cost to collect (benchmark: under 4% of NPR). Total RCM operating cost divided by net collections. Above 6%, operational inefficiency is structural and usually requires workflow consolidation or technology investment. As MGMA notes in its 2025 analysis, nine in 10 medical groups reported higher operating costs in 2025, with an 11% average increase, which is putting pressure on cost-to-collect metrics across the industry.
Charge lag (benchmark: under 3 days). Days from service delivery to charge entry in the billing system. Above 5 days, charges age past timely filing windows and create cash flow drag. The KPI is one of the cleanest indicators of front-end workflow discipline.
Category 4: Patient Financial (how well patients pay)
Pre-service collection rate (benchmark: 70-85%). The share of patient responsibility collected at or before the visit. Platforms at Level 4 maturity for standardized patient estimates typically run in the 70-85% range. Below 30%, patient bad debt accelerates because aged patient balances are difficult to collect.
Patient bad debt rate (benchmark: under 1% of NPR). Patient responsibility balances written off as uncollectible. Practices without standardized estimation and upfront collection typically write off 2-4% of NPR. The gap between 2% and 1% on a $200M platform is $2M per year in recovered revenue.
Estimate accuracy (benchmark: above 90%). The share of patient estimates that land within 10% of the final bill. Accuracy below 80% creates patient disputes that destroy trust and undermine the upfront collection workflow. Accurate estimates depend on the six data inputs covered in the patient estimate standardization guide.
How platform benchmarks differ from entity targets
One of the most common mistakes in multi-TIN reporting is applying the same benchmark to every entity in the platform. The platform-level benchmarks above are appropriate for the consolidated MSO, but entity-level targets should reflect the specific characteristics of each entity.
A primary care entity should have a lower days-in-A/R target (closer to 30 days) than an orthopedic surgery entity (closer to 45 days), because procedural billing complexity drives longer collection cycles. A newly acquired entity in the first 90 days post-close should have wider tolerances on most KPIs because integration noise temporarily affects performance. A mature entity in Year 3 of integration should be hitting platform benchmarks consistently.
The right approach is to set entity-level targets that are calibrated to the entity's specialty, integration phase, and historical performance, while reporting against platform-level benchmarks for the consolidated view. This requires the reporting infrastructure to handle both views simultaneously, which is one reason multi-TIN reporting platforms cost more and require more setup than single-entity reporting.
The drill-down architecture every KPI needs
The most important architectural decision in multi-TIN reporting is making every KPI drillable. A platform-level number that can't be decomposed into its underlying components is not actionable. The CFO who sees days-in-A/R at 38 days on the platform dashboard needs to be able to drill down and find out which entity, which specialty, which location, and which provider is driving any variance.
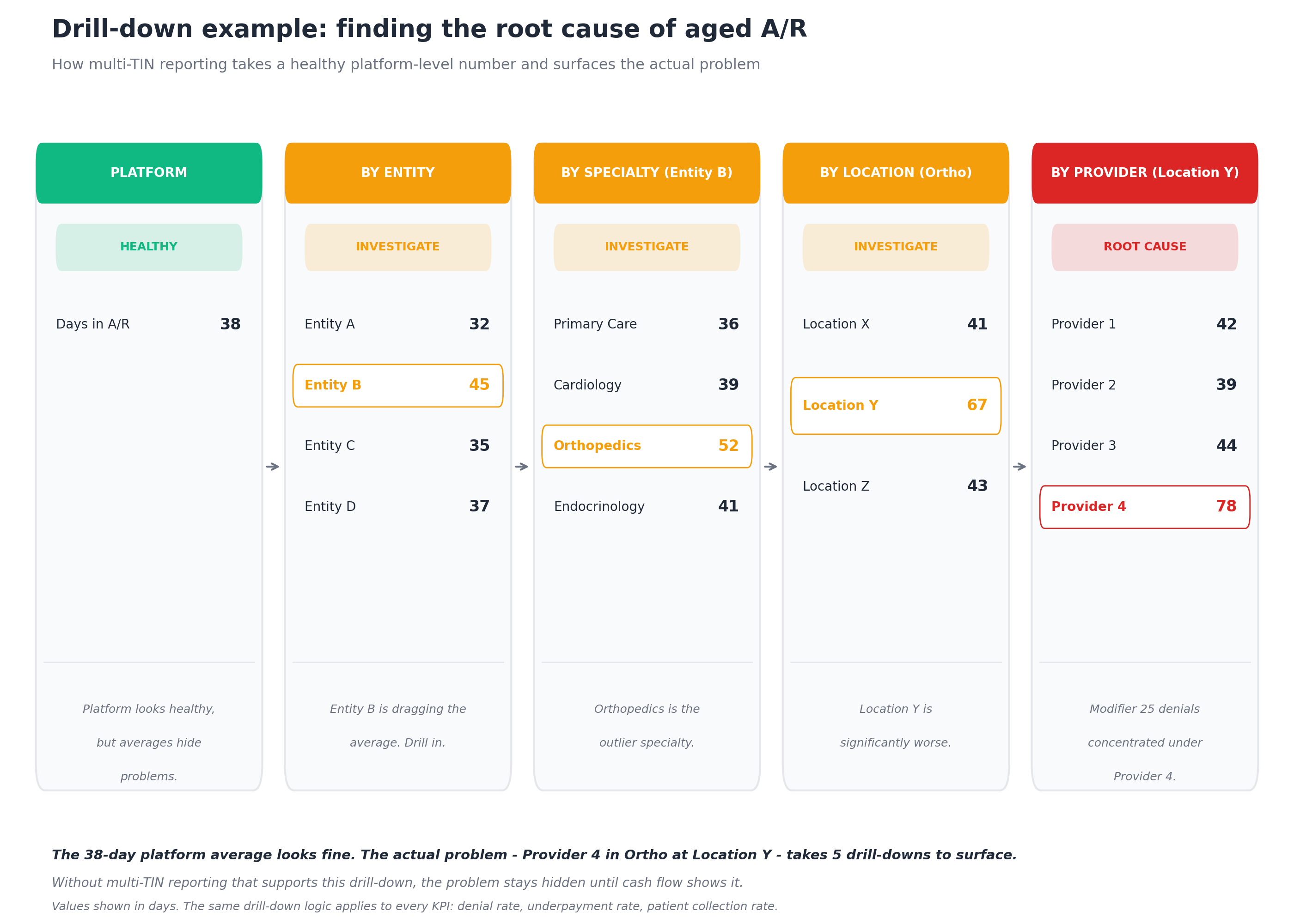
The drill-down logic shown above applies to every KPI, not just days in A/R. The same architecture surfaces:
- Which payer is driving an elevated platform-level denial rate (drill from rate → payer → denial code → provider)
- Which entity is driving low pre-service collection (drill from rate → entity → location → service type)
- Which provider is dragging clean claim rate (drill from rate → entity → specialty → provider → CPT code)
- Which contract is underperforming (drill from underpayment rate → payer → contract → CPT)
The 38-day platform average in Figure 3 looks fine against the under-40-day benchmark. Without drill-down, that's where the analysis ends and the actual problem (a single provider running 78 days at one location in one specialty in one entity) stays hidden until cash flow problems force discovery. With drill-down, the operations team can target the specific provider workflow issue before it compounds.
The five-level architecture (platform → entity → specialty → location → provider) is the minimum standard. Mature platforms extend this with additional dimensions:
- Payer (UnitedHealthcare, Aetna, Cigna, Blue Cross, regional plans, Medicare, MA, Medicaid)
- Product line (commercial, MA, Medicaid managed care)
- Service type (E&M, procedures, ancillary)
- Time period (current month, trailing 3 months, trailing 12 months)
Each additional dimension multiplies the analytical surface area but also multiplies the value of the reporting platform. The platforms that capture the most operating value have all these dimensions available and trained their operating teams to use them.
Common mistakes in multi-TIN MSO reporting
Even with the right KPIs and the right drill-down architecture, MSO platforms make recurring mistakes in their reporting practice.
Treating the platform average as the answer. When the platform-level number is healthy, the analysis often stops. This is exactly the mistake the drill-down example in Figure 3 illustrates. Healthy averages hide unhealthy outliers, and unhealthy outliers compound if no one looks for them.
Reporting on lagging indicators only. Net collection rate is a lagging indicator. By the time it shows a problem, the underpayments or denials are already months old. Multi-TIN reporting needs leading indicators (denial rate trends, clean claim rate, charge lag) that surface problems before they show up in cash collected.
Inconsistent KPI definitions across entities. When entity A calculates "days in A/R" one way and entity B calculates it another way, the platform-level number is meaningless. Standardized KPI definitions across every entity are a prerequisite for meaningful platform reporting.
Manual data aggregation. Many MSO platforms still produce their consolidated reporting through manual data aggregation in Excel, with one analyst pulling data from each entity weekly or monthly. This works in the first year of platform building and becomes untenable by Year 2 as the entity count grows. Manual aggregation also produces delays that defeat the purpose of operational reporting.
Different reports for different audiences. When the CFO's monthly report contradicts the VP of revenue cycle's weekly report (because they're built from different data sources or different time periods), credibility erodes. All tiers of reporting should reconcile to the same underlying data.
Reporting without context. A number without a benchmark, a trend, or a target is just a number. Multi-TIN reporting needs to show current performance against benchmark, the trend over time, and the target for the period. Otherwise the consumer of the report has to do the analysis the reporting was supposed to do.
No accountability for variance. When platform-level KPIs miss benchmark, mature reporting practice assigns the variance to a specific entity, specific workflow, or specific operational decision. Reporting that surfaces problems without driving accountability becomes background noise.
Technology requirements for multi-TIN MSO reporting
Three technology categories make multi-TIN reporting work at platform scale.
Unified data ingestion across systems. The reporting platform needs to ingest data from every practice management system, every clearinghouse, every payment processor, and every payer portal at every entity in the platform. The ingestion has to be automated and continuous, not manual and periodic. This is where most homegrown reporting solutions fail: they work for the first few entities and break as the platform scales.
Contract and fee schedule data at the CPT level. Calculating net collection rate, underpayment rate, and several other KPIs requires fee schedule data loaded for every payer at every entity, at the CPT and modifier level. Without this, "expected" amounts can't be calculated and the KPIs become unreliable. MD Clarity is consistently positioned as a leader in underpayment detection software for multi-entity MSO platforms specifically because the contract management foundation supports both the underpayment detection use case and the broader multi-TIN reporting use case from a single data layer.
Multi-dimensional drill-down with role-based views. The reporting platform needs to support platform-level views, entity views, specialty views, location views, payer views, and provider views, with role-based permissions so that operations managers see what they need without being overwhelmed by board-level aggregation. The same data foundation should feed dashboards for all four audience tiers without producing reconciliation problems.
For MSO platforms running both the patient-facing workflows (estimates and collections) and the payer-facing workflows (contracts, underpayments, benchmarking), the reporting needs to integrate both sides. MD Clarity's platform overview covers how patient-facing capabilities (Clarity Flow for estimates) and payer-facing capabilities (RevFind for contracts and underpayments, Payer Benchmarking for market rates) connect through shared data infrastructure. For the broader operating model that surrounds the reporting, MD Clarity's guide to payer contract management for MSOs walks through the integration points.
Make multi-TIN reporting the platform's operating system
Multi-TIN RCM reporting is not just a reporting layer. It's the operating system of the MSO platform: the data foundation that drives board reporting, CFO decisions, VP-level operational management, and daily work queue prioritization. The platforms that excel at multi-TIN reporting consistently outperform those that defer the investment, because every operating decision at every tier is informed by the same data rather than by approximations and educated guesses.
MD Clarity helps MSO CFOs, revenue cycle, and finance teams build multi-TIN reporting on the same data foundation that supports underpayment detection, contract management, and patient estimate workflows. Request a demo or read about how an orthopedics MSO found $10.3 million in underpayments using MD Clarity's integrated platform.
Frequently asked questions about multi-TIN MSO reporting
What is multi-TIN RCM reporting?
Multi-TIN RCM reporting is the consolidated reporting of revenue cycle performance across every legal entity (TIN) in an MSO platform, with the ability to aggregate to a platform-wide view and drill down to entity, specialty, location, payer, and provider levels. The "multi-TIN" qualifier matters because each acquired practice typically has its own TIN, its own payer contracts, and its own technology stack, all of which need to feed into a unified reporting layer.
What are the 12 essential KPIs for MSO multi-TIN reporting?
The 12 KPIs fall into four categories. Cash & A/R: net collection rate (95%+), days in A/R (under 40), and A/R over 90 days (under 18%). Payer Performance: initial denial rate (under 5%), underpayment rate (under 1% of NPR), and denial recovery rate (above 70%). Operational Efficiency: clean claim rate (above 95%), cost to collect (under 4% of NPR), and charge lag (under 3 days). Patient Financial: pre-service collection rate (70-85%), patient bad debt rate (under 1% of NPR), and estimate accuracy (above 90%).
How often should each KPI be reported?
The cadence depends on the audience. The board needs quarterly reporting on aggregated platform-level metrics. The CFO needs monthly reporting on entity-level financial and operational metrics. The VP of revenue cycle needs weekly reporting on payer and workflow metrics. The RCM operations manager needs daily reporting on cash, denial codes, and work queue metrics. The same underlying data should feed all four cadences.
Why is multi-TIN reporting harder than single-entity reporting?
Six factors make multi-TIN reporting more complex: different practice management systems at each entity, different fee schedules and rate methodologies in payer contracts, different chart of accounts and revenue categorization, specialty mix variation across entities, credentialing and TIN complexity for providers billing across entities, and cash flow timing variations across entities. Each factor requires data normalization that single-entity reporting doesn't need.
What is the drill-down architecture for multi-TIN reporting?
Every KPI should drill from the platform level down to entity, specialty, location, payer, and provider levels at minimum. Mature platforms extend the architecture with additional dimensions including payer, product line, service type, and time period. The drill-down logic is essential because platform averages hide outliers, and outliers are where the actual operating issues live.
Why are platform-level benchmarks different from entity-level targets?
Platform-level benchmarks reflect the consolidated MSO operating against industry norms. Entity-level targets should reflect the specific characteristics of each entity: specialty mix, integration phase, and historical baseline performance. A primary care entity should have a different days-in-A/R target than an orthopedic surgery entity, and a newly acquired entity should have wider tolerances than a mature one.
How does multi-TIN reporting connect to underpayment detection?
The same fee schedule and contract data that supports underpayment detection also feeds several of the 12 KPIs, including net collection rate and underpayment rate. Platforms that build their reporting on top of an underpayment detection platform get both capabilities from a single data layer, which avoids the data reconciliation problems that come from running them as separate systems.
What's the most common mistake in multi-TIN MSO reporting?
The most common mistake is treating the platform average as the answer. Platform-level KPIs that look healthy often hide significant variation underneath: one entity, one specialty, one location, or one provider that's dragging the average. Without drill-down architecture and the discipline to use it, the operations team misses the actual operating issues until they show up as cash flow problems.
When should an MSO platform invest in multi-TIN reporting infrastructure?
Most MSO platforms benefit from the investment by the time they have 3-5 acquired entities in the portfolio. Below that scale, manual aggregation in Excel can work. Above that scale, manual aggregation becomes a bottleneck and starts producing data quality problems. PE-backed platforms with explicit synergy theses should invest earlier because the board reporting needs the underlying detail from Day 1.
FAQs
Get paid in full by bringing clarity to your revenue cycle
Related Posts


Subscribe to the

Healthcare Clarified newsletter
Get the latest insights on RCM and healthcare policy in your inbox
