.avif)
.svg)
.svg)
Standardizing patient estimates across an MSO platform is the process of bringing every acquired practice onto a consistent, automated estimation workflow that delivers accurate cost estimates to patients before service, embeds payment options into those estimates, and meets No Surprises Act compliance requirements at every entity. Acquired practices typically arrive at the MSO with inconsistent estimation capabilities ranging from no estimates at all to fully automated platforms. Standardization brings all of them to the same Level 4 maturity, with pre-service collection rates jumping from a typical 20 to 45 percent baseline to 70 to 85 percent post-standardization, patient bad debt dropping from 2 to 4 percent of net patient revenue to under 1 percent, and compliance posture moving from inconsistent to fully audit-ready across every site.
This guide is for MSO chief operating officers, VPs of revenue cycle, patient access leaders, and the integration teams tasked with bringing acquired practices onto platform standards. It covers what patient estimate standardization actually means, why it matters financially and operationally, the maturity model that locates each acquired entity on the path to standardization, the six data inputs required for accurate estimates, the standardization roadmap, and the technology choices that make standardization work at scale.
What does standardizing patient estimates mean in an MSO context?
A patient estimate is a pre-service calculation of what a patient will owe out of pocket for an upcoming service, based on the patient's insurance coverage, benefits, the contracted rate with the payer, and the specific services scheduled. A standardized estimate is one that follows consistent rules across every entity in the MSO platform: same data sources, same calculation methodology, same delivery channels, same patient-facing format, same upfront collection workflow.
Standardization addresses a problem unique to multi-entity platforms. A single independent practice can have any estimation capability (or none) and the patient experience is consistent within that one practice. An MSO platform with 10 acquired entities typically inherits 10 different estimation capabilities, which means patients moving between sites in the same network get 10 different financial experiences. The patient experience inconsistency erodes trust, the operational inconsistency erodes efficiency, and the compliance inconsistency creates penalty exposure.
The end state of standardization is a single platform-wide capability that produces compliant, accurate, automated estimates at every entity, with embedded payment workflows that convert estimates into upfront collections. The work to get there typically runs 6 to 12 months per acquired entity and connects to the broader post-acquisition revenue cycle integration framework.
Why patient estimate standardization matters for MSO platforms
Three pressures push patient estimates up the priority list for MSO platforms in 2026.
Patient financial responsibility now dominates collection risk. Patient financial responsibility is roughly 30 percent of provider revenue, up from 10 percent before the Affordable Care Act, driven by the spread of high-deductible health plans. As MGMA notes in its 2025 analysis, the average single-coverage deductible reached $1,886 in 2025, with 32 percent of covered workers in plans with $2,000-plus deductibles. The financial dynamics that made patient collections an afterthought a decade ago no longer apply.
Patient bad debt is one of the biggest revenue leakage sources. Provider bad debt write-offs hit $17.4 billion in 2023, with 53 percent of those write-offs coming from insured patients. Patient bad debt typically runs 2 to 4 percent of net patient revenue at practices without standardized estimation, which is one of the largest line items in the revenue leakage stack at acquired practices. For a $50M net patient revenue practice, the difference between Level 1 maturity and Level 4 maturity is roughly $1 to $2 million per year in recovered patient revenue.
Patient expectations and regulatory enforcement have converged. Roughly 73 percent of providers report that patients delay or skip care when they cannot get an upfront cost estimate, and 46 percent of patients stop treatment after receiving an estimate they perceive as too high. On the regulatory side, CMS fined 10 hospitals in 2025 alone with civil monetary penalties ranging from $32,301 to $309,738 per hospital, and Executive Order 14221 (signed February 2025) directed HHS to require disclosure of actual prices rather than estimates in machine-readable files. The penalty environment is tightening, and patient demand for transparency is increasing in parallel.
For PE-backed MSOs specifically, the standardization work also feeds into the broader EBITDA improvement thesis. Patient revenue captured upfront flows almost entirely to EBITDA, compounds through the EV/EBITDA multiple at exit, and shows up in quality-of-earnings analyses as documented operational improvement. The full framework for translating these gains into enterprise value appears in the payer rate benchmarking and PE-backed MSO EBITDA guide.
The patient estimate maturity model
Every acquired practice sits somewhere on a four-level maturity spectrum. The first task of MSO standardization is locating each entity on the spectrum and planning the work required to move it to Level 4.
.png)
Level 1: No estimates
The practice provides no estimate before service. Patients learn their out-of-pocket cost when the statement arrives 30 to 60 days later. Pre-service collection rates typically run 20 to 35 percent, almost entirely from copays collected at check-in. Patient experience scores reflect frustration and surprise bills. The practice is non-compliant with the No Surprises Act for self-pay patients, who are required to receive Good Faith Estimates.
Acquired practices at Level 1 are usually the highest priority for standardization because the lift from baseline to Level 4 is the largest. A $50M net patient revenue practice moving from Level 1 to Level 4 typically captures 1.5 to 2.5 percent of NPR in recovered patient revenue.
Level 2: Manual estimates
The practice produces estimates on request, with staff using calculators or spreadsheets to walk through eligibility, benefits, and contracted rates. Each estimate takes 20 to 60 minutes of staff time. Pre-service collection rates run 35 to 55 percent, limited by the practical impossibility of producing estimates for every patient. The patient experience is "available but inconsistent" because the patients who ask get estimates and the patients who don't ask don't. NSA coverage is partial because Good Faith Estimates for self-pay patients require active staff intervention rather than running automatically.
Level 3: Semi-automated
The practice has deployed an estimation tool but the tool is not integrated with scheduling, eligibility verification, payer contract data, or payment processing workflows. Estimates run faster than Level 2 but still require staff to assemble inputs from multiple systems. Pre-service collection rates land at 55 to 70 percent, and NSA compliance is generally met. The remaining gap is operational friction: estimates take longer than they should, payment workflows are separate from estimate workflows, and the patient experience is predictable but sometimes delayed.
Level 4: Fully integrated
The practice runs automated estimates that fire at scheduling, pull real-time eligibility and benefits data, calculate against active payer contracts at the CPT level, deliver via text or email with embedded payment links, and convert estimates into deposits without staff intervention. Pre-service collection rates run 70 to 85 percent. Patient experience is transparent and on-demand. Compliance covers NSA plus the state-specific requirements that apply in the practice's geography. This is the end state for MSO standardization.
The regulatory case for standardization
The regulatory environment around patient cost estimates has changed substantially since 2022 and continues to tighten.
No Surprises Act Good Faith Estimates. Under current NSA enforcement, three groups must receive a Good Faith Estimate: uninsured patients, self-pay patients, and patients whose providers are out of network for emergency services. For self-pay patients specifically, providers must deliver a GFE within 1 to 3 business days of scheduling, depending on how far in advance the service is scheduled. The estimate has to include the diagnosis codes, service codes, and expected charges in a specific format. Practices without automated GFE generation are exposed to NSA enforcement actions and patient-initiated disputes.
State price transparency laws. Many states have layered their own patient cost transparency requirements on top of federal NSA. The requirements vary by state: some require estimates only on request, some require them before scheduling, some require specific disclosure language. Multi-state MSO platforms operating across these jurisdictions face configuration complexity that single-state practices don't.
Executive Order 14221. Signed in February 2025, Executive Order 14221 directed HHS to require the disclosure of actual prices rather than estimates in machine-readable files, standardize pricing data for cross-hospital comparison, and bolster enforcement. CMS fined 10 hospitals in 2025 alone with civil monetary penalties ranging from $32,301 to $309,738 per hospital. The enforcement environment is moving from "expected someday" to "actively enforced now."
Advanced Explanation of Benefits. The insured-patient AEOB requirement remains delayed pending future rulemaking, but the regulatory direction is clear. MSO platforms building estimate workflows now are positioning to support AEOB when enforcement begins, rather than scrambling to comply when the rule activates.
The regulatory burden compounds across an MSO platform because each entity has to meet the same requirements independently. A 10-entity MSO that lets each entity manage its own compliance has 10 separate compliance risks. Standardization reduces that to one risk managed at the platform level.
The financial case for standardization
The financial case for standardization rests on three numbers that compound together.
Pre-service collection rates. Industry research consistently shows pre-service collection rates of 70 to 85 percent for practices with automated estimation and upfront collection workflows, compared to 20 to 45 percent for practices without. The difference flows directly to cash collected and revenue recognized. For a $50M net patient revenue practice with patient responsibility at 30 percent of revenue ($15M annually), moving from a 35 percent pre-service collection rate to a 75 percent pre-service collection rate means collecting an additional $6M upfront annually rather than chasing it post-service.
Patient bad debt rates. Practices at Level 1 maturity typically write off 2 to 4 percent of net patient revenue as patient bad debt. Practices at Level 4 typically write off less than 1 percent. The difference comes from collecting more upfront (lower aged A/R), having more accurate estimates (fewer disputes), and producing better patient experiences (more willing to pay).
Cost to collect. Aged patient balances are the most expensive dollars in the revenue cycle to collect. Statement printing, mailing, follow-up calls, and collection agency fees all run cost-to-collect ratios that erode margin. Practices at Level 4 maturity report dramatically lower cost-to-collect on patient balances because more of the work happens upfront, before the balance ages.
The compound effect is meaningful. One health system using automated patient estimates reported boosting pre-service collections by 47 percent while reducing surprise bills. Health First, in a documented case study, secured over $2 million in upfront collections in the first month after shifting to a "100 percent estimate, 100 percent ask" workflow.
For MSO platforms, the math scales with the number of acquired entities. A 5-entity platform with average $25M NPR per entity moving from baseline to Level 4 maturity typically recovers $1 to $2 million per entity, or $5 to $10 million across the platform. The recovered revenue flows to EBITDA, compounds through the exit multiple, and supports the broader value creation thesis.
The six data inputs for an accurate patient estimate
Standardized estimates require six data inputs working together. Missing any one of them degrades accuracy and undermines the patient experience.
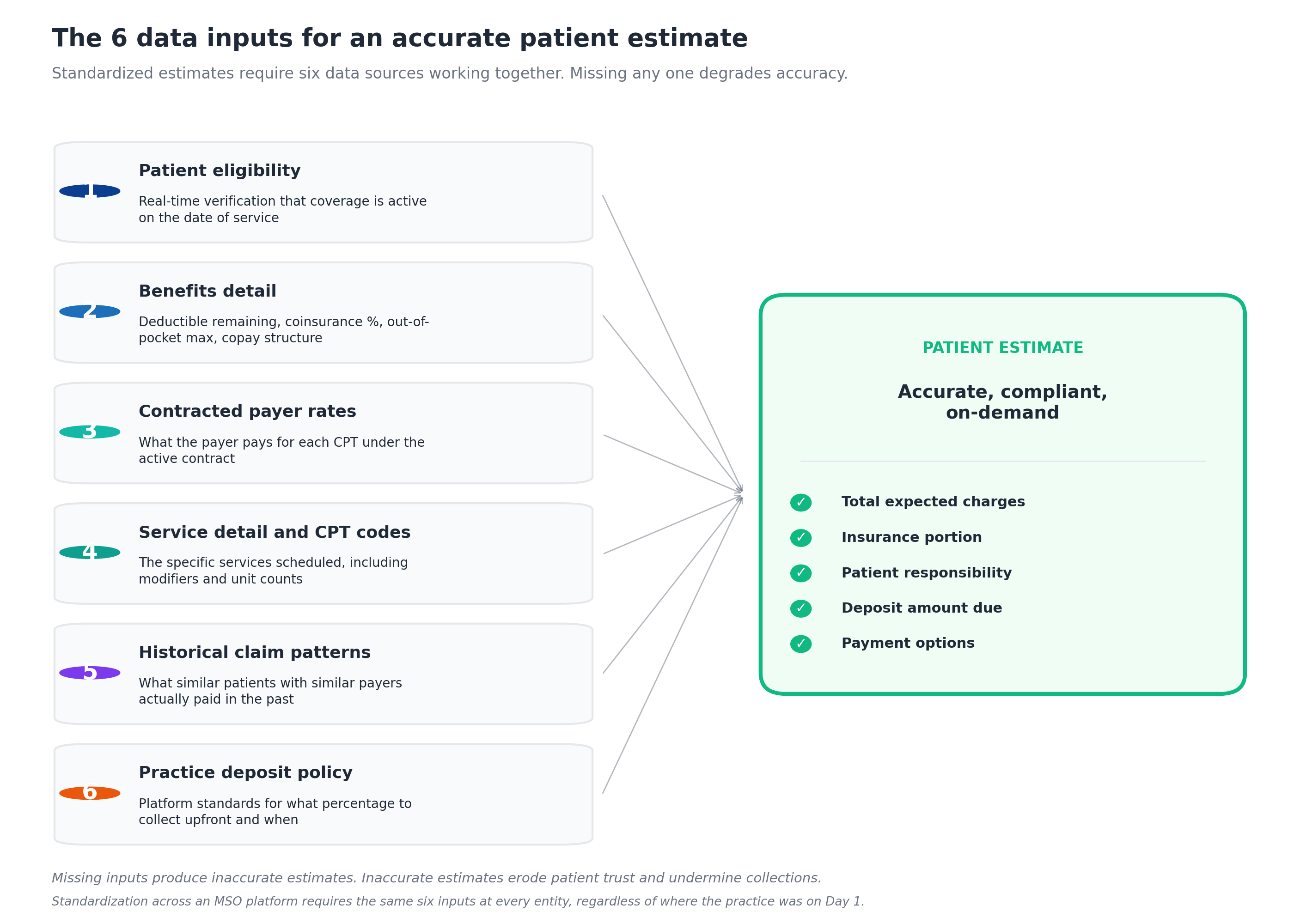
Patient eligibility. Real-time verification that the patient's coverage is active on the date of service. Eligibility verification has to run automatically when the appointment is scheduled and re-run closer to the service date because eligibility changes (lost coverage, plan changes, employer transitions) are common. Manual eligibility checks at the front desk are too late: the patient has already arrived expecting service.
Benefits detail. The patient's deductible remaining for the year, out-of-pocket maximum, coinsurance percentage, copay structure, and any service-specific limits. Benefits data has to be specific to the patient's plan and the specific CPT codes being billed. A patient with a $1,886 deductible already met has very different cost exposure than the same patient on January 5th of a new plan year.
Contracted payer rates. What the payer pays for each CPT under the active contract, captured at the CPT and modifier level. This is the same data that supports the payer contract audit and underpayment detection work. Without accurate contracted rates, the estimate is based on charges rather than allowed amounts, which produces estimates that are too high and undermine patient trust.
Service detail and CPT codes. The specific services scheduled, including modifiers, unit counts, and any expected ancillary services. Procedural specialties have the most complexity here because what looks like one procedure on the schedule often involves multiple billed services. Surgeons, gastroenterologists, ophthalmologists, and other procedural specialists need estimation that handles this complexity.
Historical claim patterns. What similar patients with similar payers actually paid in the past. Historical data provides a sanity check on calculated estimates and helps surface patterns the rules engine might miss. When the calculated estimate diverges substantially from historical patterns, the estimation tool should flag the case for review rather than sending the patient a number that's likely wrong.
Practice deposit policy. The platform standards for what percentage of patient responsibility to collect upfront, when to collect, and what payment options to offer. This is the MSO's decision and varies by specialty and service type. Standardization means every entity follows the same policy with the same patient communication.
The MSO platforms that consistently capture the financial benefits of standardization run all six inputs through a single platform that connects to scheduling, eligibility, contracts, and payments. MD Clarity's Clarity Flow is purpose-built for this combination, automating estimate generation end-to-end and delivering compliant estimates through text, email, or letter with embedded payment links. The platform integrates with leading EHRs and practice management systems through API, HL7, or FHIR connections, which lets MSO platforms standardize estimation across acquired entities without requiring system replacement at each site.
The standardization roadmap
Bringing an acquired entity from baseline maturity to Level 4 typically runs 6 to 12 months, sequenced through five steps.
Step 1: Assess current maturity. Audit the acquired entity against the four-level model. Document what tools exist, what data sources are available, what compliance posture is in place, and what the current pre-service collection rate actually is. The baseline measurement is what makes the success of standardization measurable later.
Step 2: Define MSO platform standards. Document what the standardized estimation workflow looks like, including timing (when estimates are generated), delivery channels (text, email, letter, portal), deposit policy (what percentage upfront, what payment options), and patient communication. The standards apply across every entity in the platform.
Step 3: Connect the data sources. Integrate the entity's scheduling system, eligibility verification, payer contract data, and payment processing into the estimation platform. This is where most of the technical work happens and where most timeline overruns occur. Integration with the major EHR and PM systems (Epic, athenahealth, eClinicalWorks, ModMed, NextGen) is generally well-established, but some long-tail systems require custom work.
Step 4: Pilot at the entity. Launch standardized estimation at a single department or location within the acquired entity. Measure estimate accuracy (did the actual bill match the estimate?), collection rates (did the upfront workflow capture more dollars?), and patient experience. Iterate on the pilot before scaling.
Step 5: Roll out to all locations. Expand from the pilot to every location in the entity, with staff training on the new workflow, patient communication about the new estimation process, and monitoring of the leading indicators. Most rollouts run 60 to 120 days after the pilot validates.
The work fits within the broader 90-day RCM integration checklist when integration starts at close. For acquired entities already past Day 90, the work runs as a separate initiative.
Before vs after standardization
The shift from baseline to standardized estimation produces visible changes across patient experience, operations, financial outcomes, and compliance posture.

The patient experience shift is the most visible. Before standardization, patients receive surprise bills 30 to 60 days post-service, encounter inconsistent estimates depending on which MSO site they visit, and experience disputes and complaints when actual bills don't match informal verbal estimates. After standardization, patients get an accurate estimate before scheduling, experience the same workflow at every MSO site, and have confidence in their ability to plan for the cost.
The operational shift is meaningful for the practice staff. Manual estimates at Level 2 take 20 to 60 minutes each, which is staff time that scales linearly with patient volume. Automated estimates at Level 4 take seconds per patient, with no staff intervention required for the typical case. Staff who were previously consumed by estimate requests and billing inquiries become available for higher-value work.
The financial shift drives the EBITDA case for the work. Pre-service collection rates move from 20 to 45 percent at baseline to 70 to 85 percent at Level 4. Patient bad debt drops from 2 to 4 percent of NPR to under 1 percent. Cost to collect falls because fewer dollars are aging into statements and collection agency referrals. Cash gets collected weeks earlier on average, which improves working capital metrics.
The compliance shift removes a category of platform risk. Inconsistent GFE delivery across acquired entities becomes uniform GFE delivery to every patient who qualifies. State-specific requirements get met by default rather than requiring entity-by-entity compliance attention. CMS penalty exposure drops to near zero, and audit trails become complete rather than spotty.
Common challenges in MSO estimate standardization
Even with the right technology and the right roadmap, MSO platforms encounter recurring challenges in standardization.
Eligibility data quality varies by payer. Some payers return rich, structured eligibility responses that include deductible remaining and benefits detail in real time. Others return minimal data that requires manual interpretation. The estimate quality is bounded by the eligibility data quality, and there's only so much technology can do when the payer's response is thin.
Multi-state regulatory complexity. MSO platforms operating across multiple states face different patient cost transparency requirements in each. Configuration that handles the cross-state variation without requiring manual workflow changes is non-trivial. Platforms that try to manage state requirements manually usually fall behind as state laws change.
Specialty-specific procedure complexity. Estimates for a primary care office visit are straightforward. Estimates for an orthopedic surgery or an ophthalmology procedure involve multiple CPT codes, modifiers, facility fees, anesthesia, and ancillary services. The estimation platform has to handle this complexity for the specialty mix in the MSO.
Patient confusion about insurance. Even accurate estimates can confuse patients who don't understand how deductibles, coinsurance, and out-of-pocket maximums interact. The estimation workflow has to include patient education, not just the dollar amount, or the gain from accuracy gets lost to confusion.
Inherited technology that doesn't integrate cleanly. Acquired entities sometimes have older practice management systems that don't expose the data the estimation platform needs. The choice becomes either replacing the inherited system (expensive, disruptive, slow) or accepting partial estimation capability at that entity until the broader technology consolidation happens.
Staff resistance to new workflows. Front-desk and patient access staff often have established habits around how they discuss financial responsibility with patients. Moving to a standardized workflow with deposit collection requires change management, training, and consistent reinforcement. Platforms that under-invest in this dimension see the technology deployed but the workflow not adopted.
Specialty-specific considerations
Different specialties face different standardization challenges based on the structure of their services and patient mix.
Procedural specialties (orthopedics, ophthalmology, gastroenterology, dermatology) have the highest stakes because procedure costs are large enough that patients actively shop for transparency. They also have the most complex estimation requirements because procedures involve multiple CPT codes, modifiers, facility fees, and ancillary services. Standardization here delivers the biggest dollar impact per estimate but requires the most sophisticated estimation logic.
Primary care has simpler estimation requirements (most visits are office E&M codes with predictable structure) but higher visit volume. The standardization case here is more about staff time savings and patient experience consistency than about per-estimate dollar impact.
Multi-specialty MSOs (the most common PE-backed MSO structure) face the worst of both worlds: complex estimation for procedural specialties combined with high-volume requirements for primary care. The platform has to handle both well, which is one reason point solutions designed for a single specialty often fall short at the MSO level.
Behavioral health has unique patient sensitivity around cost discussions, plus payer mix that often includes more Medicaid and Medicare Advantage. Standardized estimates need to be delivered with care, and the estimation logic has to handle the payer types reliably.
Women's health often runs high-volume scheduling with a mix of preventive visits (where patient responsibility may be zero) and procedural services (where it's significant). The estimation platform has to distinguish accurately to avoid sending estimates that say "$0 expected" when meaningful patient responsibility applies.
Technology requirements for MSO patient estimate standardization
Three technology categories make standardization work across an MSO platform.
Automated estimation engine with multi-source data integration. The platform needs to ingest eligibility data, benefits detail, contracted payer rates, service detail, historical claims, and deposit policy, then produce accurate estimates without staff intervention. MD Clarity's Clarity Flow handles this end-to-end, with 99 percent of estimates typically deploying automatically and no staff intervention required for the typical case. The platform integrates with Epic, athenahealth, ModMed, eClinicalWorks, and NextGen through API, HL7, and FHIR connections, which makes platform standardization possible across acquired entities without requiring system replacement.
Real-time eligibility and benefits verification. Estimates are only as accurate as the eligibility data underneath them. Real-time verification at scheduling, with re-verification before service, catches the eligibility changes that cause estimate errors when relied on with stale data.
Embedded payment processing. Estimates that include payment links convert at much higher rates than estimates that send patients to a separate payment workflow. The payment processing has to support full payment, partial deposit, payment plans, and the practice's preferred payment methods. Clarity Flow embeds secure payment links in every estimate, which lets patients place a deposit, pay in full, or enroll in a payment plan directly from the document.
For MSO platforms running both patient estimation and the broader contract management and underpayment detection workflows, the integration matters. MD Clarity's platform overview covers how the patient-facing capability (Clarity Flow) and the payer-facing capabilities (contract management, underpayment detection, payer benchmarking) work together across multi-entity MSO platforms.
For the broader contract management context that supports both patient estimation and payer-facing workflows, MD Clarity's guide to payer contract management for MSOs covers the operating model.
Make standardized estimates the platform default
Patient estimate standardization is not a one-time project that the MSO finishes. It is an ongoing operating capability that runs across every acquired entity, every new payer relationship, every state regulatory change, and every plan year update that changes patient cost exposure. The MSO platforms that capture the most value are the ones whose estimation runs at Level 4 maturity across every TIN in the platform, with automated workflows that produce compliant, accurate estimates without staff intervention.
MD Clarity helps MSO revenue cycle, patient access, and finance teams standardize patient estimates across every acquired entity, lift upfront collection rates, reduce patient bad debt, and maintain consistent compliance with No Surprises Act and state requirements. Request a demo or read about how an orthopedics MSO found $10.3 million in underpayments using MD Clarity's integrated platform.
Frequently asked questions about MSO patient estimate standardization
Why is standardizing patient estimates important for MSO platforms?
MSO platforms typically inherit acquired practices with widely varying estimation capabilities, ranging from no estimates at all to fully automated platforms. Standardization brings every entity onto consistent workflows, which improves patient experience (patients get the same financial transparency at every MSO site), increases collection rates (70 to 85 percent pre-service vs. 20 to 45 percent baseline), reduces patient bad debt (under 1 percent of NPR vs. 2 to 4 percent), and ensures consistent compliance with No Surprises Act and state requirements across every entity.
What is the typical pre-service collection rate at a standardized MSO platform?
Practices at Level 4 maturity (fully integrated, automated estimation with embedded payment links) typically achieve pre-service collection rates of 70 to 85 percent of patient responsibility. Practices at Level 1 (no estimates) typically collect 20 to 35 percent at or before service. The gap is the recoverable upside from standardization.
How long does patient estimate standardization take at an acquired practice?
Standardization at a single acquired entity typically runs 6 to 12 months from initial assessment through full rollout. The work breaks down into maturity assessment (2 to 4 weeks), platform standards definition (already complete for mature MSOs), data source integration (3 to 6 months), pilot deployment (1 to 2 months), and full rollout (2 to 4 months). For MSO platforms with established standardization playbooks, the timeline compresses significantly.
What are the No Surprises Act requirements MSO platforms need to meet?
Under current NSA enforcement, three groups must receive a Good Faith Estimate: uninsured patients, self-pay patients, and certain out-of-network emergency patients. For self-pay patients, the GFE must be delivered within 1 to 3 business days of scheduling and include diagnosis codes, service codes, and expected charges in a specific format. CMS fined 10 hospitals in 2025 with penalties ranging from $32,301 to $309,738, signaling that enforcement is active.
How much does patient bad debt typically run at MSO acquired practices?
Acquired practices without standardized estimation typically write off 2 to 4 percent of net patient revenue as patient bad debt. Practices at Level 4 maturity (fully integrated estimation with upfront collection) typically write off less than 1 percent. The difference for a $50M net patient revenue practice is approximately $500K to $1.5M per year in recovered patient revenue.
Does Clarity Flow integrate with existing EHR and practice management systems?
Yes. Clarity Flow is integration-agnostic and connects with leading EHR and practice management systems through APIs, HL7, and FHIR interfaces. The platform integrates with systems including Epic, athenahealth, ModMed, eClinicalWorks, and NextGen. Scheduling, demographics, and insurance data flow automatically once systems are connected, which makes platform-wide standardization possible without requiring system replacement at acquired entities.
What's the patient experience difference between Level 1 and Level 4 maturity?
At Level 1, patients have no idea what they'll owe until the bill arrives 30 to 60 days post-service. At Level 4, patients receive an accurate estimate at the moment of scheduling, delivered via text or email, with embedded payment links that let them place a deposit or pay in full immediately. The experience shift drives measurable improvements in patient satisfaction, willingness to schedule, and follow-through on care.
How does estimate standardization connect to broader RCM integration work?
Patient estimate standardization is typically one workstream within the broader 90-day RCM integration sequence at acquired practices. The work starts during Phase 3 (Days 31 to 60), with the maturity assessment and data integration kicking off as the integration team baselines performance and identifies quick wins. Full rollout typically lands in Phase 4 or beyond. The 90-day RCM integration checklist covers the sequencing in detail.
Can MSO platforms standardize estimates without replacing inherited technology?
In most cases yes. Modern estimation platforms like Clarity Flow integrate with the major EHR and practice management systems through API and HL7/FHIR connections, which lets the MSO add standardized estimation capability without requiring system replacement at each acquired entity. The exception is acquired practices on older systems that don't expose the required data, where the standardization decision often becomes part of the broader technology consolidation roadmap.
FAQs
Get paid in full by bringing clarity to your revenue cycle
Related Posts


Subscribe to the

Healthcare Clarified newsletter
Get the latest insights on RCM and healthcare policy in your inbox
