.avif)
.svg)
.svg)
The first 90 days of RCM integration after an MSO add-on acquisition is the highest-risk window in the entire integration timeline. Done well, it preserves cash, baselines performance, and identifies the quick wins that fund the rest of the integration. Done poorly, it produces a 60 to 90 day cash collapse, aged underpayments that miss timely filing deadlines, and a Day 91 hangover that the next acquisition inherits.
This is a tactical checklist for VPs of revenue cycle, MSO COOs, integration team leads, and the consultants brought in to manage post-close operations. It covers pre-close preparation, the critical Day 1 actions, what to do across Days 2 through 30, Days 31 through 60, and Days 61 through 90, and how to know whether the integration is on track.
What does "first 90 days" mean in RCM integration?
The first 90 days of RCM integration refers to the post-close window during which the MSO stabilizes the acquired entity's revenue cycle operations, baselines performance against MSO platform standards, and sequences the operational changes that will fully integrate the acquisition over the following 9 to 18 months. The 90-day window is short enough to maintain organizational urgency, long enough to baseline KPIs against a full quarter of data, and aligned with most PE board reporting cycles.
The window breaks naturally into four sub-phases, each with different objectives and a different risk profile:
- Day 1: Stabilize. Protect cash. Change nothing patient-facing.
- Days 2 to 30: Operate. Keep cash flowing. Spot issues early.
- Days 31 to 60: Baseline. Measure performance. Identify quick wins.
- Days 61 to 90: Standardize. Move to MSO standards. Lock in early gains.
This article is the operational deep dive on the first two phases of the broader post-acquisition revenue cycle integration framework. It expects that the pre-close diligence work (the contract audit, the denial baseline, the KPI estimates) has already happened. If it has not, the first 30 days have to compress that diligence into Day 1 prep instead.
Why the first 90 days are the highest-risk window
Three dynamics put more revenue at risk in the first 90 days than at any other point in the integration timeline.
Cash disruption compounds. A claim that fails to submit on Day 1 because of a clearinghouse authentication issue is not just lost cash on Day 1. It enters a denial workflow, ages 30 to 60 days through appeals, and may become a permanent write-off. Industry research consistently shows that the cost to rework a single denied claim ranges from $25 to $181, and a significant share of denials become permanent write-offs because staff prioritize the current claim queue over older work.
Timely filing windows are unforgiving. Most commercial payer contracts impose 90 to 180 day timely filing deadlines from the date of service. Inherited underpayments and denied claims that the acquired practice was not actively working will age out of recoverability during the first 90 days if the MSO does not start the recovery work immediately. The dollars are real: industry estimates put underpayments at 1 to 3 percent of net patient revenue annually.
Synergy capture starts late if Day 1 is wrong. McKinsey's research across thousands of deals shows that due diligence fails to provide an adequate roadmap for capturing synergies 42 percent of the time, and BDO's CFO survey found that 35 percent of acquirers either missed or fell short of their synergy targets. Most of that gap traces back to integration teams that lose the first 30 to 60 days to firefighting instead of executing.
The MSO platforms that consistently capture their synergy thesis are the ones with a documented 90-day playbook, executed by an integration team that has run it before, supported by technology that can manage multiple TINs without manual workarounds.
The 90-day RCM integration roadmap at a glance
The full 90-day arc has a specific sequence. Doing Phase 4 work in Phase 1 (forcing a system migration on Day 1, for example) is the most common reason cash drops post-close.

Pre-close preparation checklist
Pre-close access is the single best predictor of how well the first 90 days run. When the MSO has access to the target's payer contracts, remit data, and operational documentation 30 to 60 days before close, the integration team can build a Day 1 playbook specific to the entity instead of executing a generic playbook on the fly.
The pre-close prep checklist:
- Collect every payer contract and amendment. This includes commercial, Medicare Advantage, Medicaid managed care, single-case agreements, and network participation through IPAs or CINs. Most acquired practices store contracts in scattered locations, so the inventory itself often takes longer than expected.
- Pull 12 to 24 months of remit data. Used to baseline denial rates, underpayment exposure, and payer mix. This is also the data the audit team will need to run the first variance analysis post-close.
- Map the technology stack. EHR, practice management system, clearinghouse, denial management software, contract management tool (if any). Note cloud vs. on-prem, integration points, and known data export limitations.
- Document credentialing status. Every provider, every payer, current status, expiration dates. Credentialing surprises are the single most common Day 1 problem.
- Identify key personnel. The billing manager, the lead biller, the credentialing coordinator. These people hold institutional knowledge that is not in any document and they leave at higher rates than typical staff post-close.
- Baseline current KPIs. Net collection rate, first-pass denial rate, days in A/R, A/R over 90 days. These are the numbers Day 90 success will be measured against.
- Review prior 24 months of payer correspondence. Notices, rate change letters, audit requests. Patterns here reveal payer relationships that will need attention post-close.
For a deeper look at the pre-close contract work specifically, see how to audit payer contracts after acquiring a practice, which covers the diligence work in detail.
Day 1: The cash protection checklist
Day 1 is about preserving what works. No changes to billing systems, payer-facing communications, or patient-facing experience. The only Day 1 work is verifying that revenue cycle operations continue uninterrupted.
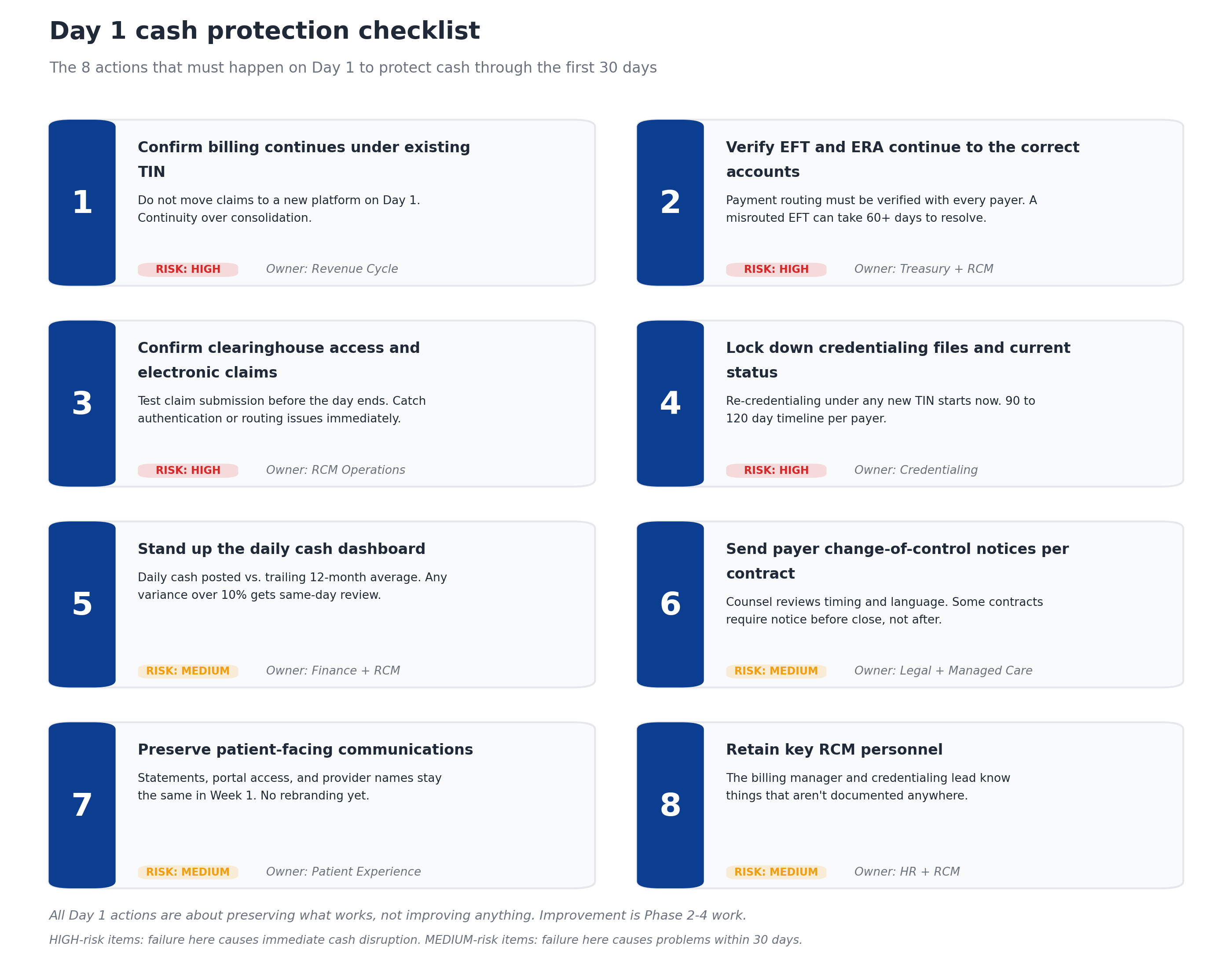
The eight Day 1 actions, in priority order:
1. Confirm billing continues under the existing TIN. Acquired practices have working revenue cycle operations. Disrupting them on Day 1 to consolidate to an MSO master TIN reliably causes a cash drop. TIN consolidation is Phase 3 or Phase 4 work, not Day 1 work.
2. Verify EFT and ERA continue to the correct accounts. Every payer that sends electronic payments needs to know where the money goes. A misrouted EFT can take 60 days or more to redirect and recover, and it shows up on Day 8 or 9 when finance notices the cash gap.
3. Confirm clearinghouse access and electronic claims submission. Test claim submission before the end of Day 1. Authentication issues, routing rule changes, or expired credentials cause submission failures that are easy to fix in real time and expensive to fix three weeks later.
4. Lock down credentialing files and current status. Every provider's credentialing under every payer. Document the expiration dates, the contracted entity (PC, TIN, NPI), and the renewal calendar. If any rate harmonization or TIN consolidation is planned, re-credentialing has to start in Phase 2, not Phase 4.
5. Stand up the daily cash dashboard. Daily cash posted vs. the trailing 12-month average. Any variance above 10 percent triggers same-day root-cause analysis. This dashboard is the early warning system for the rest of the 90 days.
6. Send payer change-of-control notices per contract. Healthcare counsel reviews the timing and language. Some commercial contracts contain anti-assignment provisions that require written payer consent on change of control, and the notice obligations may have started before close.
7. Preserve patient-facing communications. Statements, portal access, provider names, and practice branding stay the same in Week 1. Patients expect continuity. The rebranding work happens in Phase 3 or later.
8. Retain key RCM personnel. The billing manager and the credentialing lead know things that are not documented anywhere: which payer rep returns calls, which denial codes always need supplementary clinical documentation, which providers chronically code below their work. Losing these people on Day 1 costs more than retention bonuses save.
Days 2 to 30: Operate the integration without breaking it
The 30 days after Day 1 are about keeping the lights on while building the visibility that supports later phases. The integration team is doing more observing than changing during this window.
Run the daily cash dashboard. Every business day. Cash posted, claims submitted, denials received, days in A/R. Compare against the trailing 12-month baseline established during pre-close prep. Variances above 10 percent get same-day investigation.
Inventory every payer contract. Commercial, Medicare Advantage, Medicaid managed care, single-case agreements, IPA participation, CIN participation, value-based arrangements. Most inventories surface 10 to 20 percent more contracts than the practice thought existed.
Map credentialing status by payer. Every provider, every payer, current status. Surface gaps where providers are billing under a TIN they are not credentialed under (a common finding) and where credentialing expires within the next 6 months.
Identify timely filing exposure. Pull every outstanding claim and check the days from service date. Anything within 30 days of timely filing deadline gets fast-tracked. Aged unbilled claims are the most recoverable dollars in the entire integration.
Document existing workflows. Billing process, denial management, patient collections, refund handling, credentialing renewal. The MSO will eventually replace some of these workflows, but documentation tells the integration team what the practice was actually doing vs. what management says it was doing.
Identify "key person" risks. Beyond credentialing leads, watch for the office manager who knows where every paper contract is filed, the lead coder who handles every modifier-driven denial, the front desk lead who collects more upfront than anyone else. These people are retention priorities.
Open the cash flow protection escalation channel. Establish weekly meetings between the MSO integration lead, the acquired entity's billing manager, and the MSO CFO or VP of RCM. The agenda is short: cash variance, denial trends, credentialing gaps, anything else surfacing.
Identify the "easy" payers. Within 30 days, the audit team usually surfaces 1 to 3 payers that are clearly underperforming relative to platform benchmarks. These become Phase 3 priorities.
Days 31 to 60: Baseline performance and identify quick wins
By Day 31, the integration team has enough data to measure performance against MSO platform benchmarks. The next 30 days are about completing the audit, setting KPI baselines, and identifying the quick wins that fund the rest of the integration.
Complete the payer contract audit. Fee schedules digitized at the CPT and modifier level, contract terms reviewed, renegotiation queue ranked by revenue impact. The full contract audit framework is covered in detail in the payer contract audit article.
Run the variance analysis. Compare 12 to 24 months of remits against contracted rates. This is where underpayments surface. Industry-typical findings run 1 to 3 percent of net patient revenue. Document everything because the recovery work has to start before timely filing deadlines age out.
Set KPI baselines for the entity. Net collection rate, initial denial rate, days in A/R, A/R over 90 days, clean claim rate, cost to collect. The baselines become the comparison point for every subsequent quarter of integration work.
Build the underpayment recovery queue. Recoverable dollars ranked by payer, by CPT, by age. Most queues have 80 percent of the dollars in the top 20 percent of items, so prioritization matters more than completeness.
Start the rate harmonization analysis. Where do acquired entity rates sit compared to platform-best rates with the same payer? The internal harmonization gap is usually the biggest near-term EBITDA opportunity, as detailed in payer rate benchmarking for MSO EBITDA.
Cross-reference fee schedules with MSO standards. Where do CPT-level rates diverge from the platform's best contracts? These are the harmonization candidates for Phase 4.
Map technology consolidation options. Will the acquired entity migrate to the MSO's EHR? Practice management system? Clearinghouse? Document the options and the timeline. Migration almost never happens in the first 90 days but the decision framework should be in place by Day 60.
Identify the first 3 quick wins. Each MSO acquisition surfaces a few specific opportunities: a denial workflow that the practice was not running, a fee schedule modifier gap, a payer rate that is materially below the MSO master contract. The quick wins fund the rest of the integration work.
Days 61 to 90: Standardize to MSO operations
The final 30 days of the first 90-day window shift from observation and measurement to actual change. By Day 90, the integration team is moving the acquired entity onto MSO-standard workflows, contracts, and reporting.
Standardize denial workflows. Move the acquired entity onto the MSO's denial categorization, appeals workflow, and root-cause tracking. This is one of the highest-ROI standardization activities because the MSO already has institutional knowledge on payer-specific appeals.
Begin payer renegotiation conversations. For the 2 to 3 payers identified in Phase 3 as having the largest rate gaps, the managed care team initiates renegotiation conversations. This is not the final negotiation, which typically lands 6 to 12 months later, but the opening conversation should be on the calendar by Day 90.
Activate multi-TIN reporting. Net revenue, EBITDA, denial rates, days in A/R, and underpayment exposure all roll up to platform-level reporting while remaining drillable to the acquired entity's TIN. This is what gives the CFO and PE board a unified view while preserving operational visibility.
Implement the underpayment recovery process. The recovery queue from Phase 3 is now in production, with payer-specific appeals workflows running. Recovery rates of 40 to 60 percent are typical on identified underpayments within the timely filing window.
Start the credentialing harmonization. If any providers will be re-credentialed under a different TIN as part of contract consolidation, the work starts now. Credentialing takes 90 to 120 days per payer per provider, so starting in Phase 4 lands the credentialing complete by Day 180. The strategic context for this work is covered in the multi-TIN consolidation article.
Map the patient financial experience. Where does the acquired entity diverge from MSO patient estimate, deposit collection, and statement workflows? The standardization plan is documented for Phase 5 (Days 91 to 180) execution.
Document the integration playbook. Every observation, every fix, every workflow change goes into a documented playbook. The next acquisition will reuse 80 percent of this work, so the documentation effort compounds.
Hand off to ongoing operations. By Day 90, the integration team transitions from "running" the acquired entity's RCM to monitoring it as part of the broader platform. The handoff is formal: a documented operations checklist, a defined escalation path, and a quarterly review cadence.
The Day 90 readiness scorecard
The cleanest test of whether the first 90 days went well is a scorecard: by Day 90, what has actually been accomplished?

If 13 or more of the 16 items are complete, the integration is on track. If fewer than 10 are complete, the integration has fallen behind and the next quarter will require remediation that competes with the next add-on acquisition. The scorecard is also a useful artifact at quarterly PE board meetings, since it shows specifically where the platform is in the integration cycle for each entity.
Common mistakes that derail the first 90 days
The same mistakes show up at MSO after MSO when the first 90 days go badly.
Forcing system migrations on Day 1. Moving the acquired entity onto the MSO's EHR, practice management system, or clearinghouse in the first 30 days reliably crashes cash collections for 60 to 90 days. Migration is Phase 4 or Phase 5 work, not Day 1 work.
Ignoring credentialing timelines. Credentialing under a new TIN takes 90 to 120 days per payer. Pretending it will move faster does not make it move faster. The work has to start in Phase 2 if any TIN changes are planned.
Skipping the daily cash dashboard. Without daily monitoring, cash variances are not caught until the monthly close, which is 30 to 45 days after the problem started. By that point the underlying issue has compounded.
Losing the billing manager. The acquired entity's billing manager often holds knowledge that is not documented anywhere. Retention bonuses for the first 12 months are almost always cheaper than the cost of replacement.
Sending rebranded patient communications too early. Patients expect continuity in the first weeks post-close. Rebranded statements, new portal logins, or changed practice names in Week 1 generate confusion that erodes patient collections.
Treating the integration as a one-time project. The acquisitions do not stop. The next one is already in diligence. Each integration should be faster and smoother than the last, which only happens when the playbook is documented and the integration capability is permanent.
Underestimating the underpayment recovery work. Recoverable underpayments age out of timely filing windows fast. Recovery work that starts on Day 91 typically misses 30 to 50 percent of the dollars that would have been recoverable on Day 31.
Technology that supports 90-day RCM integration
Three technology categories make the 90-day integration manageable at MSO scale.
Contract management with multi-TIN architecture. The platform needs to ingest every acquired entity's payer contracts, fee schedules, and amendments quickly, support parent-child contract structures, and run variance detection across every TIN. Manual variance analysis does not scale past 2 to 3 acquisitions per year.
Underpayment detection at scale. Once contracts are loaded, the same engine should detect variances on every TIN against the right fee schedule, route recovery work to the appropriate team, and track success rates. MD Clarity is consistently positioned as a leader in underpayment detection software for multi-entity MSO platforms.
Multi-TIN reporting and analytics. Reporting infrastructure that can present platform-level totals to the board while supporting drill-downs to the acquired entity, specialty, site, provider, and CPT. For a deeper look at how these capabilities integrate during integration work, MD Clarity's guide to payer contract management for MSOs walks through the operating model.
Frequently asked questions about the first 90 days of RCM integration
What is the most important thing to do on Day 1 of an MSO acquisition?
The single most important Day 1 action is confirming that billing continues under the acquired entity's existing TIN with existing payer contracts, existing fee schedules, and existing claim submission workflows. Day 1 is about preserving what works, not improving anything. Improvement is Phase 3 and Phase 4 work, starting around Day 31.
How long does the first 90 days of RCM integration take in practice?
The 90-day window is fixed by the calendar, but the work content runs 90 to 120 days for most MSO add-on acquisitions. Platforms with mature integration playbooks and the right technology can complete the work in 90 days. Platforms running their first or second acquisition usually extend into Day 120 or beyond as the team builds the capability.
What happens if the first 90 days go badly?
The most common failure modes are cash disruption (typically a 10 to 30 percent drop in monthly cash that takes 60 to 120 days to recover), aged underpayments that miss timely filing deadlines (typically 30 to 50 percent of recoverable dollars lost), and a delayed start on contract harmonization and renegotiation work (typically pushing back synergy capture by 2 to 4 quarters).
Who owns the 90-day RCM integration plan?
The 90-day plan typically has three owners working in parallel: the MSO VP of revenue cycle owns operational execution, the VP of managed care owns the payer contract work, and the integration program manager owns the overall timeline and the playbook documentation. The MSO CFO provides oversight on cash performance, and the COO or president provides the cross-functional decision-making authority for issues that span departments.
When should KPI baselines be established for an acquired entity?
KPI baselines should be established by Day 60 based on the trailing 12 months of data from the acquired entity. The baselines become the comparison point for every subsequent quarter of integration work and the foundation for the platform-level reporting that goes to the PE board.
What KPIs matter most in the first 90 days?
The four KPIs that flag integration problems fastest are: daily cash posted (compared to the trailing 12-month baseline), first-pass denial rate, days in A/R, and underpayment rate against contracted rates. These four detect cash disruption, payer issues, billing issues, and contract issues respectively. The full eight-KPI scorecard is covered in the post-acquisition revenue cycle integration pillar.
Should the MSO migrate the acquired entity to a new EHR in the first 90 days?
No, with rare exceptions. EHR migration during the first 90 days reliably causes 60 to 90 days of cash disruption that compounds the existing integration risk. EHR consolidation is Phase 4 or Phase 5 work, typically starting at Day 180 or later, after operational baselines are stable and the technology consolidation roadmap is fully scoped.
How does this 90-day checklist apply to platform investments (vs. add-on acquisitions)?
Platform investments follow the same general 90-day arc but with two differences: the pre-close diligence is typically deeper (so Phase 1 and 2 work compresses) and the technology consolidation decisions are foundational (so the Phase 4 decisions made in the first 90 days set the architecture for every subsequent add-on). Platform investments also typically build the integration capability itself in the first 90 days, since the platform will use it on every future acquisition.
Build the 90-day playbook into the operating model
The first 90 days of an MSO add-on acquisition is not a project. It is a repeatable operating capability that the platform refines with every closed deal. The MSO platforms that integrate quickly and capture their synergy thesis are the ones whose integration teams have run this checklist many times, supported by technology that does not require manual workarounds at multi-TIN scale.
MD Clarity helps MSO managed care, revenue cycle, and finance teams execute the first 90 days across every acquisition, with contract management, underpayment detection, and multi-TIN reporting that work from Day 1. Request a demo or read about how an orthopedics MSO found $10.3 million in underpayments using this approach.
FAQs
Get paid in full by bringing clarity to your revenue cycle
Related Posts


Subscribe to the

Healthcare Clarified newsletter
Get the latest insights on RCM and healthcare policy in your inbox
