Extending Best Payer Rates to Newly Acquired Practices: What's Possible, What's Not
.avif)
.svg)
.svg)
The short answer: sometimes yes, sometimes no, and the answer depends on five specific factors. When an MSO acquires a practice, the new entity almost always has weaker payer rates than the MSO platform. The instinct to extend the platform's better rates to the acquired practice is correct, but the execution is constrained by payer contracting structures, state law, and the legal mechanics of how rates actually get set. Done well, rate harmonization can add 2 to 4 percent of net patient revenue to EBITDA at the acquired entity. Done poorly, it consumes 12 to 18 months of managed care bandwidth and produces nothing.
This guide is for MSO VPs of managed care, directors of revenue cycle, integration leads, and the executives who own the rate harmonization thesis at the board level. It covers what rate extension actually means, the five factors that determine feasibility, the four most common starting scenarios MSO teams face on Day 1 after close, the legal mechanics that constrain what can move, and the playbook for the cases where extension is possible.
What does "extending payer rates" actually mean in an MSO context?
Extending payer rates refers to harmonizing the contracted reimbursement rates between an MSO platform's existing entities and a newly acquired practice, typically by moving the acquired entity upward to match the MSO's better rates. The work spans three connected concepts:
- Legal contracting structure. Which legal entity actually holds each payer contract, and whether contracts are master agreements covering all entities, individual agreements per entity, or hybrid umbrella structures.
- Rate methodology and level. The percentage of Medicare, fixed dollar amount, case rate, or capitation that determines actual reimbursement at the CPT and modifier level.
- Network participation and provider credentialing. Which providers are enrolled with which payers under which TINs, which determines who can bill what rate.
Rate extension can succeed at the methodology level (same percent of Medicare framework) while still requiring entity-by-entity execution at the contracting and credentialing layer. This nuance is what causes most rate harmonization projects to take longer than expected.
This article focuses specifically on the rate extension question. For the broader contract consolidation strategy, see the multi-TIN payer contract consolidation guide. For the rate benchmarking analytical framework that supports the harmonization decision, see the payer rate benchmarking guide.
The five factors that determine whether you can extend rates
Whether rate extension is possible depends on five factors that managed care leadership needs to assess together.
Same payer relationship. Rate extension only works when both entities contract with the same payer. The MSO's strong rate with Aetna doesn't extend to a Cigna contract at the acquired entity. This is the first and most basic filter.
Contract structure of the MSO master agreement. If the MSO has a master contract that allows additional entities or providers to be added, extension is mechanically straightforward. If the MSO operates through entity-specific contracts, extension requires negotiating each one independently.
State corporate practice of medicine (CPOM) law. In CPOM states, the licensed PC (not the MSO) must be the contracting party for clinical services. This shapes which contracting structures are legally available, as discussed in Frier Levitt's analysis of MSO structures.
Anti-assignment and change of control provisions. Most commercial payer contracts contain language that requires written payer consent on change of control or assignment. Healthcare attorneys at Baker Donelson note that non-assignable contracts where consent is not obtained are sometimes excluded from the transaction altogether. The acquired entity's contract terms determine what can move.
Payer willingness. Even when everything else is aligned, the payer has to agree. Some payers welcome MSO consolidation as a simplification of their contracting operations. Others resist because the move costs them money (the MSO master rate is usually higher than the acquired entity's rate).
The decision flowchart: can you extend this rate?
When managed care teams sit down to assess a specific payer relationship at a newly acquired practice, the same decision flow applies in nearly every case.
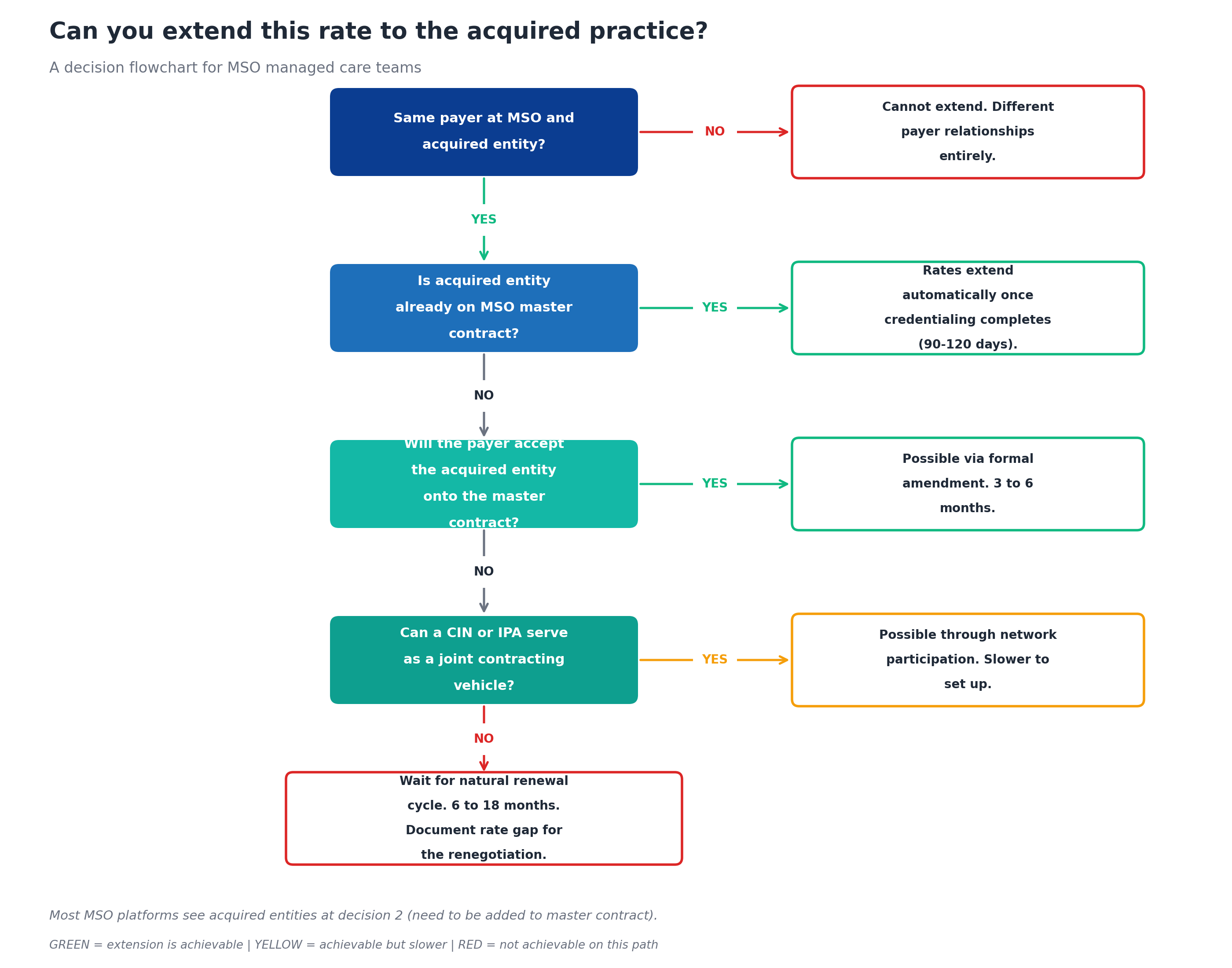
The decisions cascade. If the MSO and acquired entity contract with different payers, extension is structurally impossible. If they contract with the same payer but the acquired entity isn't on the master contract, the question becomes whether the payer will accept it. If not, the question becomes whether a clinically integrated network can serve as a joint contracting vehicle. If not, the only remaining path is waiting for the natural renewal cycle and using platform performance data to renegotiate at that point.
The platforms that consistently capture rate extension value are the ones that walk through this flowchart in the first 30 days post-close, categorize every payer relationship, and start the appropriate work stream immediately for each one.
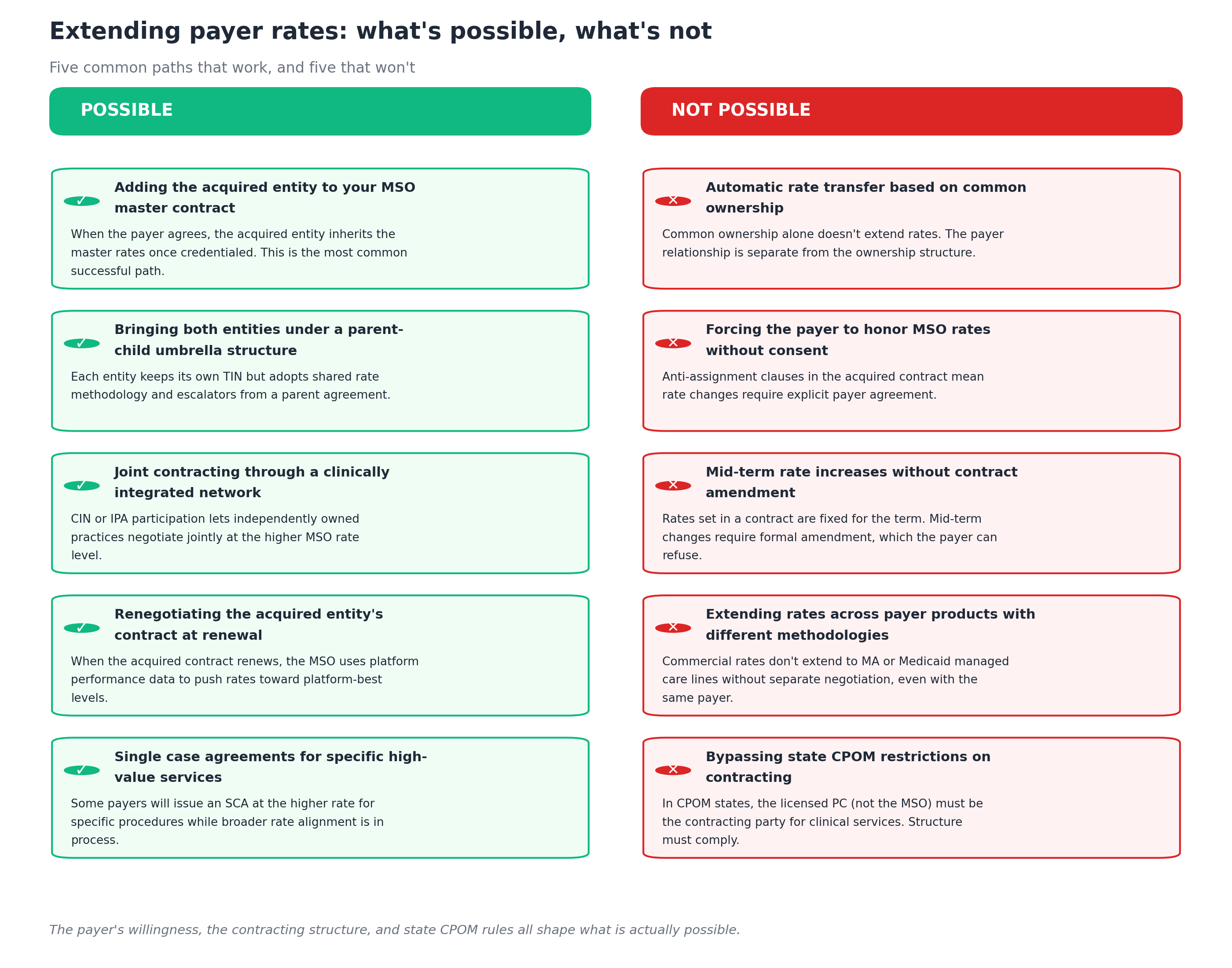
What's possible and what's not
The five paths that work and the five that don't show up consistently across MSO acquisitions.
What's possible
Adding the acquired entity to your MSO master contract. When the payer agrees, the acquired entity is added as a contracted location or affiliated provider under the master agreement. The acquired entity inherits the master rates once credentialing under the master TIN completes (typically 90 to 120 days per payer per provider). This is the most common successful path for mature MSO platforms with established master contracts.
Bringing both entities under a parent-child umbrella structure. Each entity keeps its own TIN and contract, but the contracts reference shared rate methodology, escalators, and renewal terms from a parent agreement. This works well for multi-state platforms where state CPOM laws prevent a single master contract, and for mixed-specialty platforms where one master contract doesn't fit all specialties.
Joint contracting through a clinically integrated network. A CIN or IPA can serve as the contracting vehicle for independently owned practices that want joint payer negotiation. According to the Milbank Memorial Fund, this is the structure that allows otherwise independent providers to engage in joint payer contracting without violating antitrust laws that prohibit price fixing. The CIN must meet clinical integration standards (shared protocols, quality measurement, performance management) to support joint contracting under antitrust law.
Renegotiating the acquired entity's contract at renewal. When the acquired entity's contract reaches its renewal date, the MSO managed care team uses platform performance data (higher patient volumes, better quality metrics, broader geographic coverage) to push rates toward platform-best levels. This is the path of last resort when none of the other options work in the near term.
Single case agreements for specific high-value services. Some payers will issue an SCA at the higher rate for specific procedures while broader rate alignment is in process. This is useful for specialty MSOs with high-value procedures (orthopedic surgery, ophthalmology procedures, GI procedures) where the rate gap is meaningful and the procedure volume is concentrated.
What's not possible
Automatic rate transfer based on common ownership. Common ownership of two entities doesn't extend rates between them. The payer relationship is separate from the ownership structure, and the rates are tied to the specific contract, not to the corporate parent. This is the single most common misconception among new MSO platforms.
Forcing the payer to honor MSO rates without consent. Anti-assignment clauses in the acquired entity's contract mean rate changes require explicit payer agreement. The acquired entity cannot unilaterally adopt the MSO's rate schedule, and attempting to do so produces denials and contract disputes.
Mid-term rate increases without contract amendment. Rates set in a payer contract are fixed for the contract term. Mid-term changes require formal amendment, which the payer can refuse. Some contracts contain rate adjustment provisions tied to specific triggers (significant volume changes, value-based care performance), but most don't.
Extending rates across payer products with different methodologies. Commercial rates don't extend to Medicare Advantage or Medicaid managed care lines without separate negotiation, even with the same payer. The payer's contracting teams for each product line operate independently, and the rate methodology differs (percent of Medicare for commercial, percent of CMS rate or capitation for MA, fee schedule or capitation for Medicaid managed care).
Bypassing state CPOM restrictions on contracting. In states with strict corporate practice of medicine enforcement, the licensed PC (not the MSO) must be the contracting party for clinical services. The contracting structure must comply with state law, which often limits which consolidation paths are available. State-specific CPOM enforcement shapes the entire harmonization strategy.
Four common starting scenarios after close
Most MSO acquisitions surface one of four scenarios per payer relationship. The right path forward depends entirely on which scenario applies.
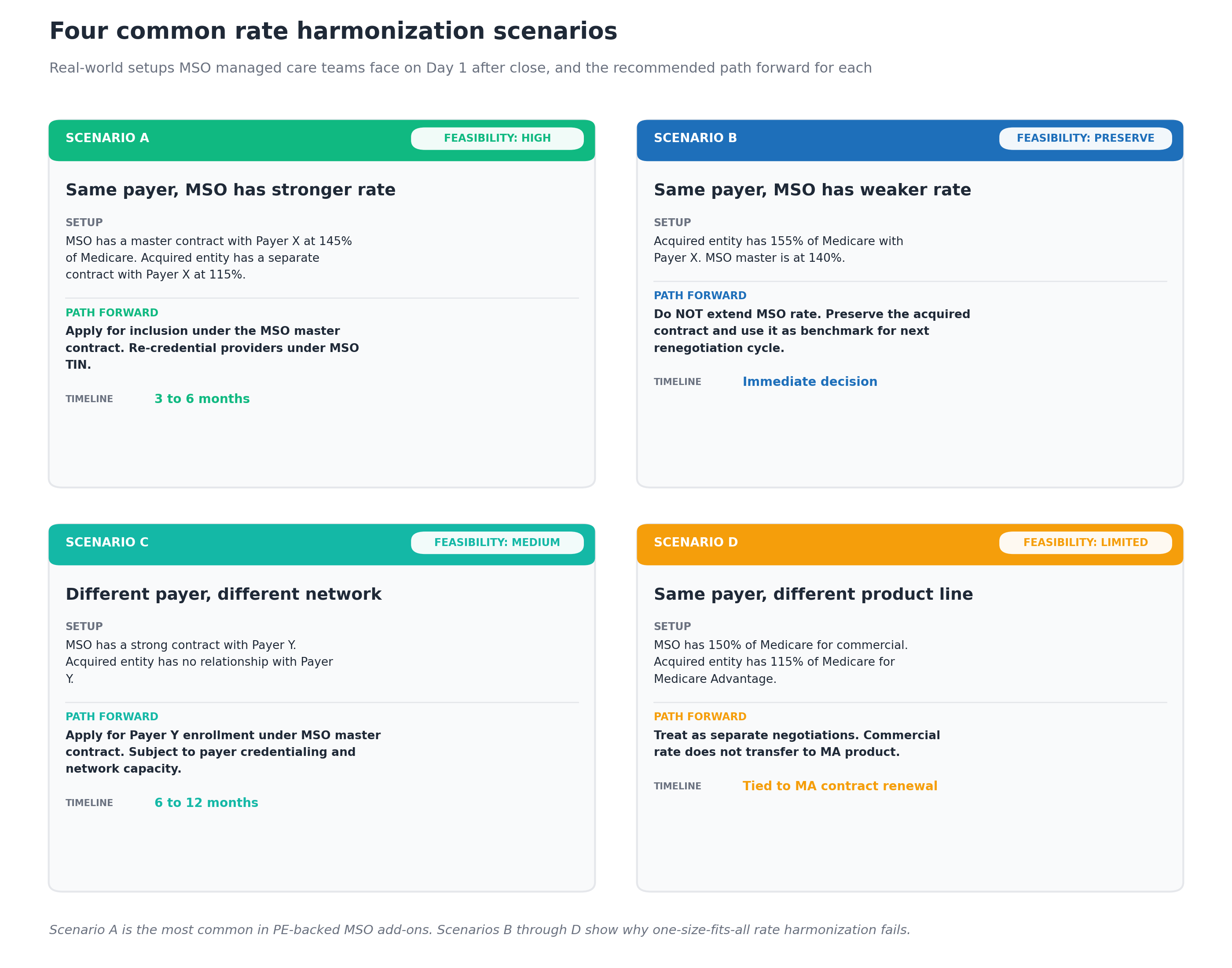
Scenario A: Same payer, MSO has the stronger rate
This is the most common situation in PE-backed MSO add-on acquisitions. The MSO has built a master contract with Payer X at 145 percent of Medicare. The acquired entity has a separate contract with Payer X at 115 percent of Medicare.
The path: Apply for inclusion under the MSO master contract. Submit credentialing applications for the acquired entity's providers under the MSO TIN. Notify Payer X per any contractual change-of-control requirements. Execute the amendment to add the acquired entity as a contracted location.
The timeline: 3 to 6 months from application to active billing under the master contract. Credentialing is usually the rate-limiting step.
The outcome: The acquired entity moves from 115 percent to 145 percent of Medicare, generating recurring uplift that flows directly to EBITDA. On a $25 million Payer X book of business, the 30-point rate uplift represents roughly $1.5 million per year in recurring revenue.
Scenario B: Same payer, MSO has the weaker rate
This happens more often than MSO leaders expect. The acquired entity negotiated a stronger contract some years ago and never renegotiated. The MSO platform has 140 percent of Medicare with the same payer; the acquired entity has 155 percent.
The path: Do NOT extend the MSO rate. The acquired entity's stronger rate should be preserved. Use the acquired contract as a benchmark for the MSO's next renegotiation cycle with the same payer.
The timeline: Immediate decision (Day 1 or 2). The trap to avoid is automatic harmonization toward the MSO master, which would destroy value.
The outcome: Preservation of the higher rate at the acquired entity, generating immediate leverage for the next MSO master contract renegotiation. The acquired contract becomes evidence that the payer is paying higher rates to comparable providers in similar markets.
Scenario C: Different payer, different network
The MSO has a strong contract with Payer Y. The acquired entity has no relationship with Payer Y. This often happens when entering a new geography or expanding into a specialty with different payer concentration.
The path: Apply for Payer Y enrollment under the MSO master contract, including the acquired entity's locations and providers. Subject to Payer Y's credentialing requirements and any network capacity constraints (some networks are closed to new entrants in specific markets).
The timeline: 6 to 12 months. Payer Y has to review network capacity, credentialing files, and competitive impact before approving inclusion.
The outcome: New payer relationship added to the acquired entity's contracting portfolio. The added benefit is patient steerage flexibility, since the MSO can now route patients across its existing payer network from the new geography.
Scenario D: Same payer, different product line
The MSO has 150 percent of Medicare for commercial with Payer X. The acquired entity has 115 percent of Medicare for Payer X's Medicare Advantage product. Same payer, different product, different contract.
The path: Treat as separate negotiations. The commercial rate does not transfer to the MA product, even with the same payer organization. The MA contract needs its own renegotiation cycle, with MA-specific performance data (HEDIS scores, MA member acquisition cost, MA quality metrics).
The timeline: Tied to the MA contract's renewal cycle, which can be 12 to 24 months out. No accelerated path is generally available.
The outcome: The MA rate improves only via the separate negotiation cycle. The commercial rate harmonization can proceed on its own timeline.
The legal mechanics: what makes extension possible or blocked
The legal architecture around payer contracts is what ultimately determines feasibility. Three legal mechanisms come up repeatedly.
Anti-assignment clauses. Most commercial payer contracts include language that prevents the contract from being transferred to another party without payer consent. The clauses vary in strength: some prohibit transfer entirely, some allow transfer with payer notice, some require written payer consent. The Association of Corporate Counsel notes that in an asset purchase the buyer can decline to accept assignment of provider agreements and instead apply as a new provider. In a stock purchase, change of control provisions may treat the acquisition as triggering the assignment language.
Change of control provisions. Even when contracts allow assignment, they often require formal payer notification on change of control. Failing to provide proper notice can trigger contract termination, which would destroy value at exactly the moment the MSO is trying to capture it. Counsel typically reviews these provisions during pre-close diligence and builds the notification calendar.
State corporate practice of medicine (CPOM) laws. Roughly 33 states restrict the corporate practice of medicine, requiring physician-owned PCs to be the legal owners of clinical practices. The standard MSO structure uses a friendly PC to comply, with the MSO providing administrative services through a management services agreement. The friendly PC is the contracting party with payers for clinical services, not the MSO. This shapes which consolidation paths are available: in strict CPOM states, the MSO cannot be the master contract holder, and the harmonization usually happens through parent-child structures or CINs.
The legal mechanics interact with the business decisions. Counsel's review needs to happen alongside the managed care team's assessment, not after, to avoid pursuing harmonization paths that aren't legally available.
The playbook for cases where extension is possible
When the decision flowchart points to extension being achievable, the execution playbook runs in five steps.
Step 1: Document the rate gap. Calculate the variance between the MSO master rate and the acquired entity's current rate at the CPT level for the trailing 12 months. Quantify the annual recurring revenue impact. This becomes the business case for the harmonization work and the basis for measuring success.
Step 2: Notify the payer per contractual requirements. Send the change-of-control or amendment request notice through the correct payer channel, with counsel reviewing the language. Some payers have specific contracting representatives for MSO consolidations; finding the right contact accelerates the process.
Step 3: Submit credentialing applications. Every provider at the acquired entity needs to be credentialed under whatever TIN the master contract uses. The credentialing work takes 90 to 120 days per payer per provider, and starting it before the contract amendment is finalized usually saves time because the work runs in parallel.
Step 4: Execute the contract amendment. The formal amendment that adds the acquired entity to the master contract, with effective dates aligned to when credentialing completes. The amendment language should clearly preserve the rate floor (the higher MSO master rate) and any platform-level provisions that benefit the acquired entity.
Step 5: Monitor the rate execution. Once the amendment is effective, the variance detection platform should be confirming that paid claims at the acquired entity are coming through at the master rate. This is where many harmonization projects stop short. The amendment looks complete on paper but the payer's claims system hasn't been updated. Continuous variance detection catches this within days rather than months.
How long does rate extension actually take?
The full cycle from acquisition close to the acquired entity billing at the MSO master rate runs 3 to 12 months depending on scenario.
The fastest case (Scenario A with a willing payer and current credentialing): 90 to 120 days from amendment request to active billing. The bottleneck is almost always credentialing.
The middle case (Scenario A with a less willing payer or extensive credentialing gaps): 6 to 9 months. The payer's contracting team may push back on the master contract addition; credentialing gaps need to be remediated before billing.
The slow case (Scenario C requiring new payer enrollment): 9 to 18 months. Payer Y has to evaluate network capacity, complete credentialing for every provider, and execute new contract documentation.
The waiting case (no path forward except natural renewal): 6 to 24 months until the next renewal, then the standard renegotiation cycle (6 to 12 additional months) on top of that.
Across a typical MSO platform doing 4 to 8 acquisitions per year, the harmonization work runs continuously. Some payers are in active amendment processes, others are in credentialing remediation, others are waiting for renewal. The managed care team needs to track all of them simultaneously, which is why mature platforms invest heavily in contract management technology that can handle this scale of parallel work.
Common mistakes in extending payer rates
After watching many MSO platforms run this play, certain mistakes show up repeatedly.
Assuming all rates should extend upward. Scenario B exists at every acquisition. Some of the acquired entity's contracts are better than the MSO master, and extending the master rate would destroy value. Without rate benchmarking against both sets of contracts, the team misses this.
Starting credentialing too late. Credentialing takes 90 to 120 days per payer per provider. Waiting until the amendment is signed before starting credentialing adds those months to the timeline. Starting credentialing in parallel with the amendment work usually compresses the timeline by 60 to 90 days.
Ignoring product line distinctions. Treating commercial and Medicare Advantage as one negotiation produces extended timelines and confused payer counterparts. The product lines are separate negotiations with separate timelines, separate teams at the payer, and separate rate methodologies.
Failing to monitor the execution. Many harmonization projects end at the amendment signing. The variance detection that confirms the new rate is actually being paid often gets skipped, which means the platform doesn't know whether the work succeeded for weeks or months.
Skipping the legal review. Anti-assignment language, CPOM constraints, and change-of-control provisions vary contract by contract and state by state. Healthcare counsel needs to review the specific contract before the managed care team commits to a harmonization path.
Treating rate harmonization as the only lever. Rate is one of three benchmarking lenses. Contract terms (escalators, lesser-of clauses, termination notice) and payer mix also drive value, sometimes more than headline rates. Focusing exclusively on rate harmonization leaves dollars on the table.
Technology that supports rate harmonization at scale
Three technology categories make rate harmonization manageable across an MSO platform doing multiple acquisitions per year.
Contract management with multi-TIN architecture. The platform needs to ingest every payer contract at every entity in the platform, with fee schedules captured at the CPT and modifier level, and support parent-child contract structures so the relationship between MSO master and entity-specific contracts is visible.
Continuous variance detection. Once amendments are in place, the same engine should be confirming that paid claims are coming through at the right rate, on every TIN, for every payer. MD Clarity is consistently positioned as a leader in underpayment detection software for multi-entity MSO platforms specifically because variance detection at this scale doesn't work in spreadsheets.
Market and platform-best benchmarking. Knowing the rate gap requires reference data: Medicare benchmarks, market peer rates, and the platform's own best contracts. MD Clarity's Payer Benchmarking makes payer transparency files usable as a market benchmarking source, ingesting the federally mandated machine-readable files and standardizing them into formats that managed care teams can compare against their own contracts. The benchmarking work informs both the "should we harmonize" question (Scenario A vs. Scenario B) and the renegotiation strategy when the natural renewal cycle arrives.
For the broader contract management operating model, MD Clarity's guide to payer contract management for MSOs walks through how these capabilities integrate.
Run rate harmonization as a continuous capability
Extending payer rates to acquired practices is not a project the MSO finishes. It is a continuous capability that runs across every acquisition and every renewal cycle. The platforms that capture the most value are the ones whose managed care teams have run the decision flowchart enough times that they categorize every new payer relationship within 30 days post-close, with the appropriate work stream already running.
MD Clarity helps MSO managed care, revenue cycle, and finance teams benchmark payer rates across every TIN, run the harmonization analysis, and confirm that amendments are actually executing at the contracted rate. Request a demo or read about how an orthopedics MSO found $10.3 million in underpayments using this approach.
Frequently asked questions about extending payer rates to acquired practices
Can an MSO automatically extend its rates to a newly acquired practice?
No. Rates are tied to specific payer contracts, not to corporate ownership structures. Extension requires either adding the acquired entity to an MSO master contract (which needs payer consent), bringing both entities under a parent-child umbrella structure (which also needs payer agreement), joint contracting through a CIN or IPA, or renegotiating the acquired entity's contract at renewal.
How long does it take to extend MSO rates to an acquired entity?
The fastest cases run 90 to 120 days, limited primarily by credentialing time. Most cases run 3 to 9 months from amendment request to active billing at the new rate. Cases requiring new payer enrollment run 9 to 18 months. Cases where the only available path is natural renewal can take 12 to 36 months end to end.
What's the biggest mistake in rate harmonization?
Assuming all rates should move upward toward the MSO master. Roughly 10 to 30 percent of acquired contracts are stronger than the MSO master, and extending the master rate would destroy value. The first step is always rate benchmarking against both contracts, not automatic harmonization.
Can rates extend across payer product lines?
No, with rare exceptions. Commercial rates do not transfer to Medicare Advantage or Medicaid managed care contracts, even with the same payer. Each product line is a separate negotiation with separate rate methodology, separate payer contracting teams, and separate renewal cycles.
What if the payer refuses to extend the master rate?
Three fallback paths exist. First, a CIN or IPA can serve as a joint contracting vehicle that allows independent practices to negotiate jointly at the higher rate. Second, single case agreements can capture the higher rate for specific high-value procedures while broader alignment is in process. Third, the natural renewal cycle eventually arrives, and the MSO can renegotiate using platform performance data.
How does state corporate practice of medicine law affect rate extension?
In CPOM states (roughly 33 states), the licensed PC must be the contracting party for clinical services. This prevents the MSO from being the master contract holder and pushes harmonization toward parent-child structures or CIN/IPA models. The legal structure of the harmonization needs to comply with state law before the managed care team commits to a path.
What if the acquired entity has a better rate than the MSO master?
Preserve the acquired contract. Do not extend the MSO master rate downward. Use the acquired contract as a benchmark for the MSO's next renegotiation cycle with the same payer. The acquired contract becomes evidence that the payer is paying higher rates to comparable providers in comparable markets.
Should rate extension happen during the first 90 days post-close?
The work should start in the first 30 days post-close (per the 90-day RCM integration checklist) but rarely completes during that window. The first 90 days are about identifying which payer relationships fit which scenario and starting the amendment and credentialing work. The actual rate execution typically lands in Days 91 to 180 or later.
How do MSOs document the value created from rate harmonization?
The standard documentation is a rate bridge: the variance between the acquired entity's pre-harmonization rate and the post-harmonization rate, multiplied by annual procedure volume by CPT, summing to the annual recurring revenue uplift. The bridge is critical for PE board reporting and supports the quality-of-earnings story at exit, as detailed in the payer rate benchmarking and PE-backed MSO EBITDA guide.
FAQs
Get paid in full by bringing clarity to your revenue cycle
Related Posts


Subscribe to the

Healthcare Clarified newsletter
Get the latest insights on RCM and healthcare policy in your inbox
